How AI is changing the business model, not just the care model
One of the more important developments in behavioral health is that AI is not only expanding what can be delivered digitally; it is also broadening how vendors get paid. Historically, many behavioral health solutions relied on a relatively simple model: direct-to-consumer subscriptions, employer-paid access fees or reimbursed clinical encounters. That model is becoming more layered. As AI tools are embedded earlier in the patient journey and across more channels, revenue increasingly can be captured at multiple points — at the population level through employer or health plan contracts, at the engagement layer through digital navigation and self-guided support, and at the clinical tier when a member steps up into coaching, therapy, psychiatry or other covered services. These models are not always mutually exclusive at the life level; in practice, the same individual may sit inside multiple sponsored benefit channels at once, so the same covered life may be monetized more than once across the ecosystem.
This is creating a model that looks increasingly familiar to anyone who has followed employee assistance program (EAP) evolution: A broad population may be covered through an embedded or access-based contract, but only a subset engages deeply enough to generate additional utilization, referral or care-management revenue. AI can make that structure more powerful by serving as the always-on front door — identifying need earlier, improving engagement, routing people to the right level of care and keeping members active between visits. In that sense, AI is not only a clinical tool; it is also a conversion, retention and care-navigation layer. The same covered life may therefore be monetized sequentially across multiple offerings, especially when the vendor sits inside the carrier, employer or provider workflow. Rather than a standardized industry rule, this is an inference from how many current offerings are being structured.
The market is already moving in this direction. Spring Health pairs an employer-facing EAP+ model with broader platform services and has also expanded its behavioral health platform to more health plans. Lyra markets a single platform across employers and health plans, combining guided self-care, provider matching, coaching, therapy, medication support and AI-enabled tools. Headspace continues to position itself with health plans through a mix of content, digital support and provider-backed care. Wysa, meanwhile, spans employers, insurers, health systems and primary-care-linked pathways, using AI self-help and navigation to engage users and then route them onward to other services when appropriate. The implication is that the winning business models may be those that combine low-cost, population-level reach with the ability to capture higher-value clinical experiences, navigation assistance and workflow revenue as needs intensify.
For buyers, that makes vendor evaluation more complex. It is no longer enough to ask whether an AI tool “works.” The better question is whether the vendor’s commercial model aligns incentives across access, engagement, escalation and outcomes. Solutions that monetize only at the point of high-acuity clinical use may struggle to justify broad deployment. By contrast, models that combine access fees, embedded distribution, and step-up care revenue may have stronger economics and more room to invest in safety, evidence generation and workflow integration over time.
What could slow adoption
The barriers to adoption are real and should be treated as structural rather than temporary. Clinical risk is the most obvious one. Behavioral healthcare includes situations involving suicidality, other self-harm, trauma, psychosis and rapid decompensation. A system that performs well most of the time but fails badly in edge cases is not ready for broad deployment. Safety, therefore, is not just a product issue; it is a market access issue.
The evidence base is another limiter. Early signals are promising, and formal research activity is increasing, but many stakeholders will still want more proof before they treat AI-enabled behavioral support as clinically interchangeable with human care. Dartmouth’s early Therabot trial is an important indication that more rigorous evidence is starting to emerge, but one encouraging study certainly does not indicate a broad clinical consensus. Payors, in particular, are likely to remain cautious until evidence, practice guidance and payment pathways mature further. Employers may move somewhat faster in lower-risk use cases, especially as more guided-support pilots come to market, but they too will need confidence that innovation is not outrunning governance.
Provider acceptance will also shape the curve. Clinicians are broadly receptive to tools that reduce burden and improve continuity, but many remain skeptical of tools that threaten therapeutic quality, professional responsibility or the therapeutic alliance itself. Their skepticism is not an obstacle to be brushed aside. It is a useful design constraint. The strongest products will be the ones that make clinicians more effective, not the ones that assume trust can be bypassed.
Finally, the policy environment is beginning to move from abstract concern to real governance. As formal frameworks, state-level reviews and best-practice guidance develop, the field will become easier to evaluate but harder to bluff. Utah’s 2026 regulatory experience is one example of how quickly the discussion can shift from general AI enthusiasm to concrete inquiries around disclosures, escalation and consumer protection in mental health settings. That is a healthy shift. In a domain this sensitive, discipline is likely to be a precondition for adoption rather than a brake on it. Beyond clinical risk and evidence, reimbursement remains a gating mechanism. Until AI-enabled interventions are recognized within formal payment models, adoption will remain constrained regardless of technical progress.
What to watch over the next three to five years
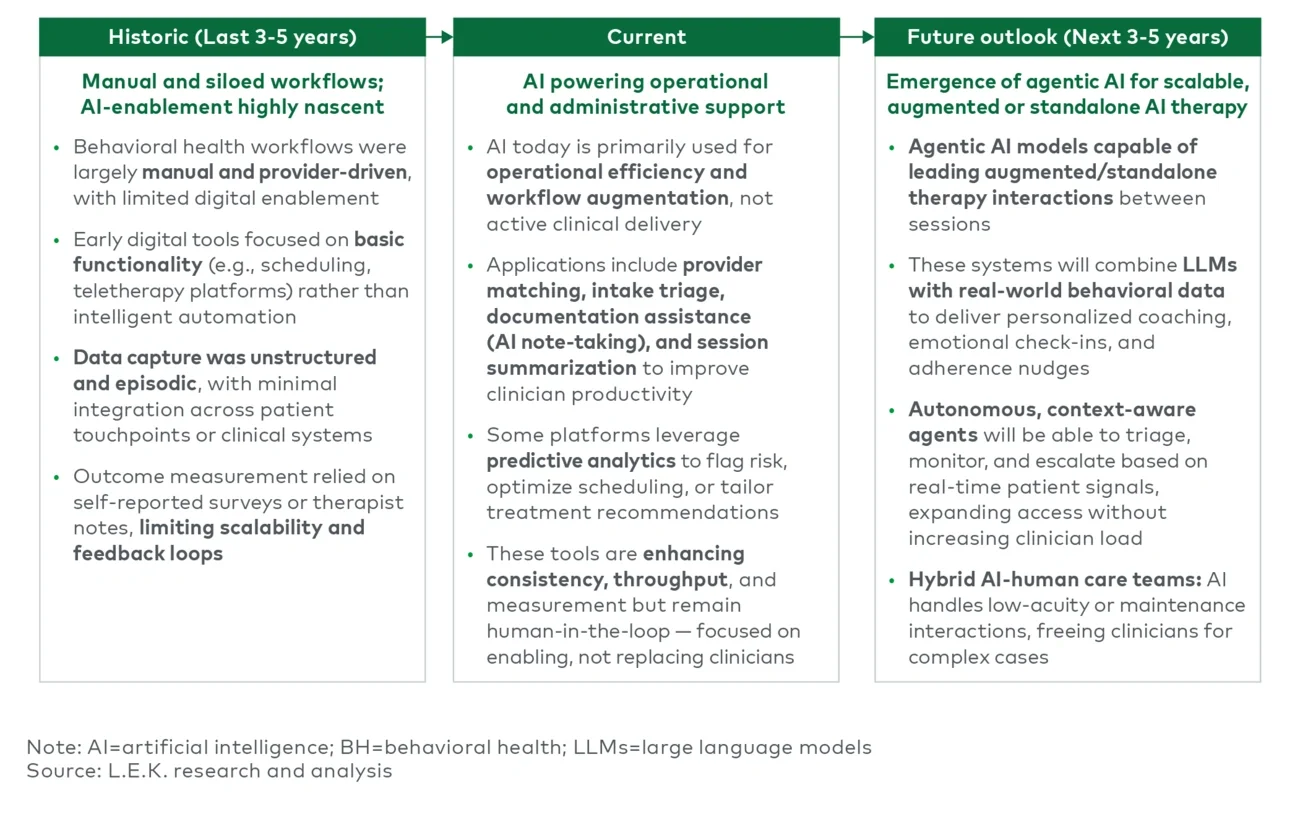
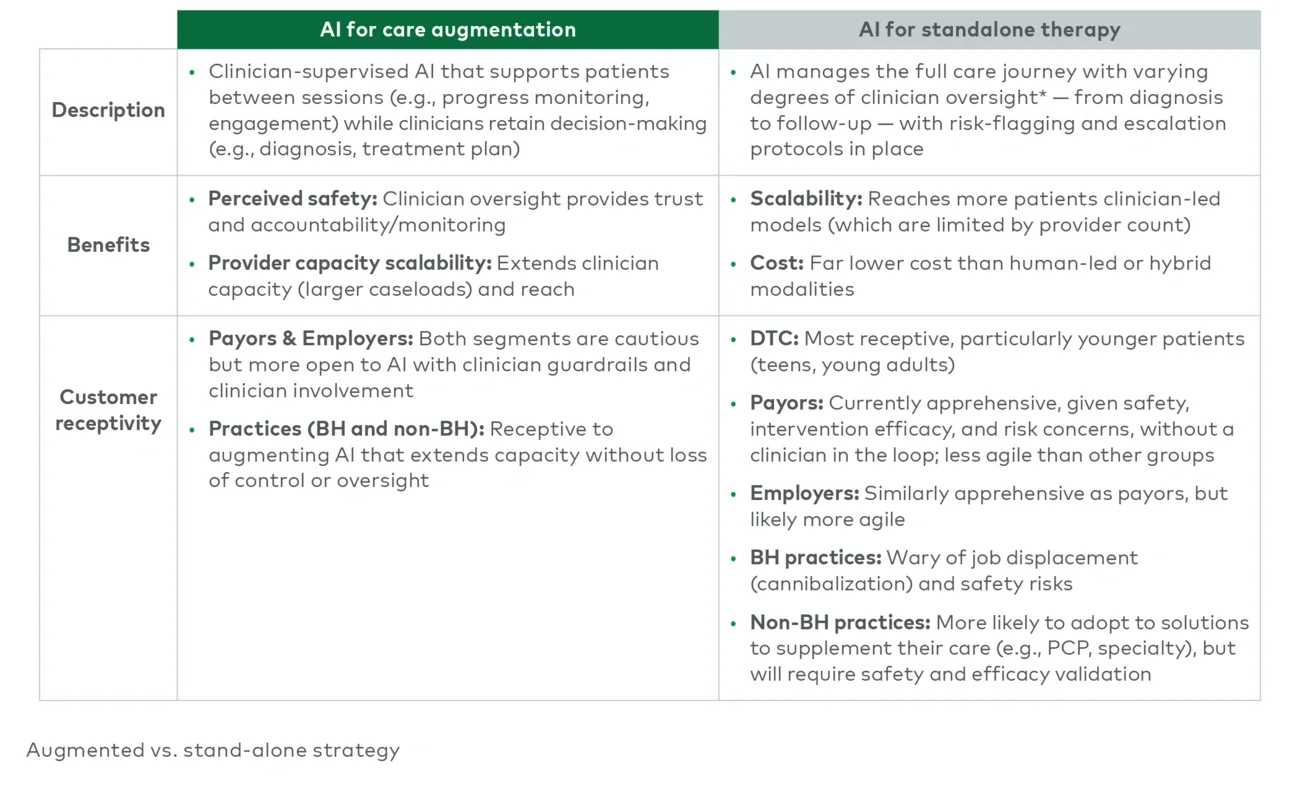
The most likely near-term outcome is that augmentation will become the norm before autonomy becomes mainstream. AI will become more common in intake, engagement, measurement, documentation and lower-intensity support. At the same time, a smaller set of bounded autonomous use cases will continue to be tested, especially in lower-acuity settings or in direct-to-consumer channels where the need for always-available support is especially visible.
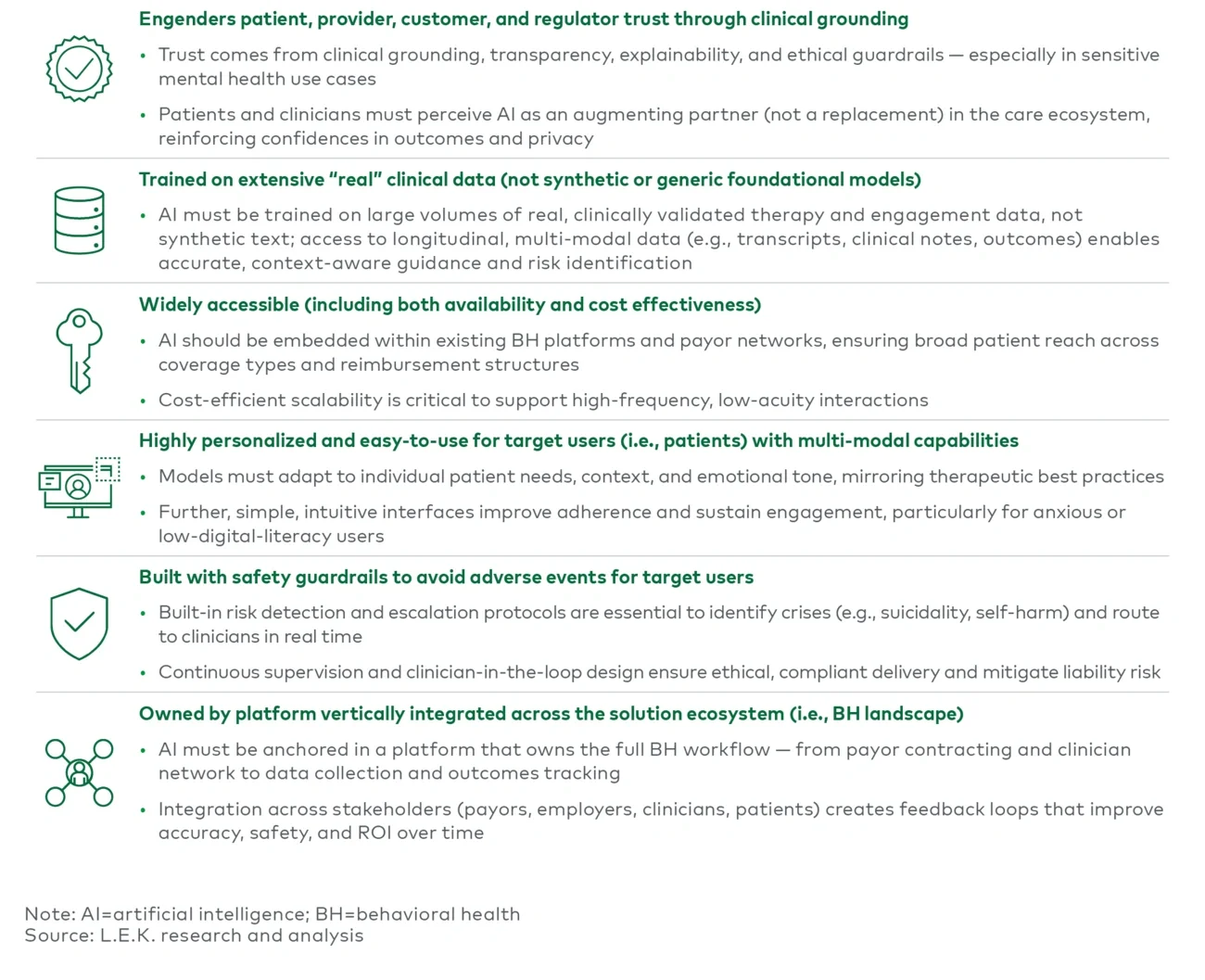
Several signals will determine whether the market moves faster. One is evidence: More clinical trials, stronger real-world outcomes, and clearer differentiation between low-risk wellness tools and clinical-grade interventions are required. Another is regulation: This means practical standards for disclosure, escalation, documentation and accountability — not necessarily heavy-handed regulation. A third is reimbursement: Once payment models better recognize AI-supported or AI-mediated care, adoption could accelerate meaningfully. A fourth is institutional trust: As more buyers see rigorous guardrails, transparent evaluation and credible oversight, it will become easier to move from pilot to scaled deployment.
For the broader market, the implication is clear: AI will matter in behavioral health, but the issue is not simply whether it works. The real questions ask where it can be trusted, how it will be governed and which organizations can combine product capability with clinical credibility. The market is now moving out of the broad curiosity phase and into the phase of selective proof. That is exactly where serious categories begin to take shape.
A related implication is that the most attractive behavioral health models may be those with multiple monetization layers around the same covered population. In practical terms, that can mean pairing carrier-embedded or employer-paid access revenue with AI-enabled navigation, step-up referral, claims-based clinical care, and in some cases provider-facing workflow tools or analytics. As in EAP, breadth of covered access matters — but the real strategic advantage may come from owning the member journey across multiple points of engagement and escalation.
Conclusion
Behavioral health is one of the clearest real-world tests for AI: Can it improve care in a way that is both scalable and responsible? The need is urgent, the economics are supportive and the digital fit is stronger than in many other areas of healthcare. But it is also a category in which harm, if it occurs, will be highly visible and deeply consequential.
That is why the future is unlikely to belong to the boldest claims. More likely it will belong to the most disciplined models — those that improve access without overreaching, extend clinician capacity without eroding judgment, and create more continuous support without losing sight of safety, evidence and trust. Over the next several years, the center of the market will likely move toward AI-enabled hybrid care. The organizations that succeed will be the ones that treat trust not as a communications issue but as part of the product itself. Over time, the sector’s leaders may be distinguished not only by clinical outcomes and safety, but also by their ability to build resilient, multilayered business models around access, engagement, escalation and longitudinal member value.
For more information, please contact us.
L.E.K. Consulting is a registered trademark of L.E.K. Consulting LLC. All other products and brands mentioned in this document are properties of their respective owners. © 2026 L.E.K. Consulting LLC