SLE disease complexity
Systemic lupus erythematosus (SLE) is a complex multisystem immune condition where a patient’s immune system becomes dysregulated and produces autoantibodies, leading to widespread inflammation and innate immune activity. The impact of the disease is profound, with the vast majority of patients developing complex symptomatology and facing reduced life expectancy.
Diagnosing and treating SLE continues to present substantial challenges due to its unpredictable natural history and broad range of clinical manifestations. Symptoms can vary drastically between patients — ranging from joint pain and fatigue to severe organ failure. Symptoms often overlap with other diseases as well. Along with current limitations in diagnostic tests, disease mischaracterization can delay diagnosis and lead to varied patient management and suboptimal care. Today, it can take almost six years between initial SLE symptom onset and formal diagnosis. On top of the difficulty with diagnosis, the disease’s heterogeneity also means no single treatment plan will fit all patients, and therapeutic effectiveness may vary greatly based on disease severity and comorbidities. If untreated or managed incorrectly (including delayed treatment), SLE patients can experience organ failure, such as kidney failure (commonly beginning as lupus nephritis) and heart failure.
Utilization of real-world data — such as healthcare claims — can provide greater clarity on current SLE management practices across diverse patient groups and provide SLE-focused drug manufacturers with a set of data-driven outputs that can support strategic planning. Ultimately, better characterization of treatment dynamics enables manufacturers to align their strategies with unmet needs in a way that enhances both patient outcomes and commercial success.
Patient natural history, SLE diagnosis and comorbidity presence
Recent SLE patient diagnosis and treatment dynamics were evaluated through the Komodo Healthcare Map® claims database from 2016 to 2024. To evaluate the differential diagnosis dynamics among SLE patients, a cohort of SLE patients from the Komodo dataset was defined as individuals who had multiple SLE claims at least four years apart (i.e., patients with a higher likelihood of “true’’ SLE diagnosis). This identified roughly 270,000 unique individuals, with a 9:1 distribution of women to men. Approximately 30% of these SLE patients were identified as having a misdiagnosed illness at some point during their SLE diagnosis journey. Almost half of these misdiagnoses were for common diseases with overlapping SLE symptoms.
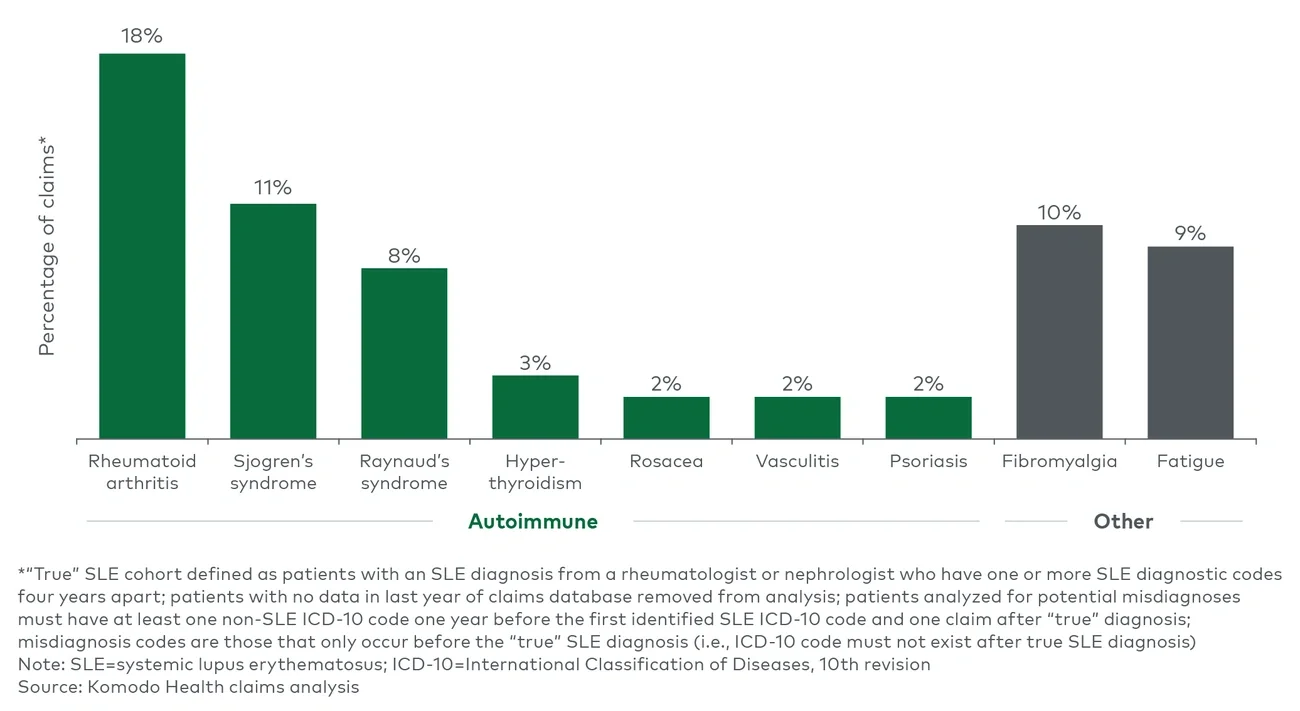
Both autoimmune diseases and non-autoimmune diseases with prominent SLE symptom overlap were identified as the most frequent misdiagnoses claims codes in the SLE patient cohort (see Figure 1). Overlapping symptoms such as joint pain, dry mouth and fatigue appear to contribute to misdiagnosis. In select cases, these overlapping symptoms can be indicative of a combined manifestation of both diseases (e.g., secondary manifestation of Raynaud’s syndrome in SLE patients).
The range of possible misdiagnoses likely contributes to the longer diagnostic journey and treatment mismanagement commonly experienced by SLE patients, as healthcare providers must decipher and treat symptoms without being able to determine the underlying cause. In cases such as fibromyalgia and fatigue, treatment options may vary drastically from what is prescribed to SLE patients — as healthcare providers focus on treating the pain and fatigue instead of the underlying inflammation. In autoimmune misdiagnosis situations, there may be overlap in initial nonspecific immunosuppressant treatments (e.g., disease-modifying anti-rheumatic drugs (DMARDs)) but no overlap in more specific treatment options targeting the underlying biology of SLE.