Patient-centric delivery has a confidence problem
For nearly a decade after biosimilar competition entered the pegfilgrastim market, Neulasta Onpro retained approximately half the U.S. market and protected a segment that Coherus estimated to be worth approximately $1.2 billion. The product’s differentiation was not based on the molecule, formulation or price. It was based on delivery.
The on-body injector automated administration within a narrow post-chemotherapy dosing window, removing the need for patients to self-manage a time-sensitive treatment decision while recovering from therapy. Its value came from eliminating complexity and uncertainty.
This example highlights a broader shift occurring across drug delivery. While patient-centricity is often associated with reducing pain, anxiety and injection burden, many of the most successful delivery innovations have instead focused on increasing patient confidence that treatment is being administered correctly.
As self-administration becomes more common across biologics and specialty therapies, understanding the sources of patient uncertainty is becoming increasingly important for development teams seeking to improve adherence, persistence and treatment outcomes.
Patient-centricity is about resolving uncertainty
The conventional view of patient-centric delivery focuses on comfort-related improvements such as smaller needles, lower injection force, reduced viscosity and less injection-site pain. These factors matter and can influence patient preference.
However, evidence from human factors research and real-world use suggests that correct administration is often determined by whether patients can confidently navigate the treatment process outside the clinical environment.
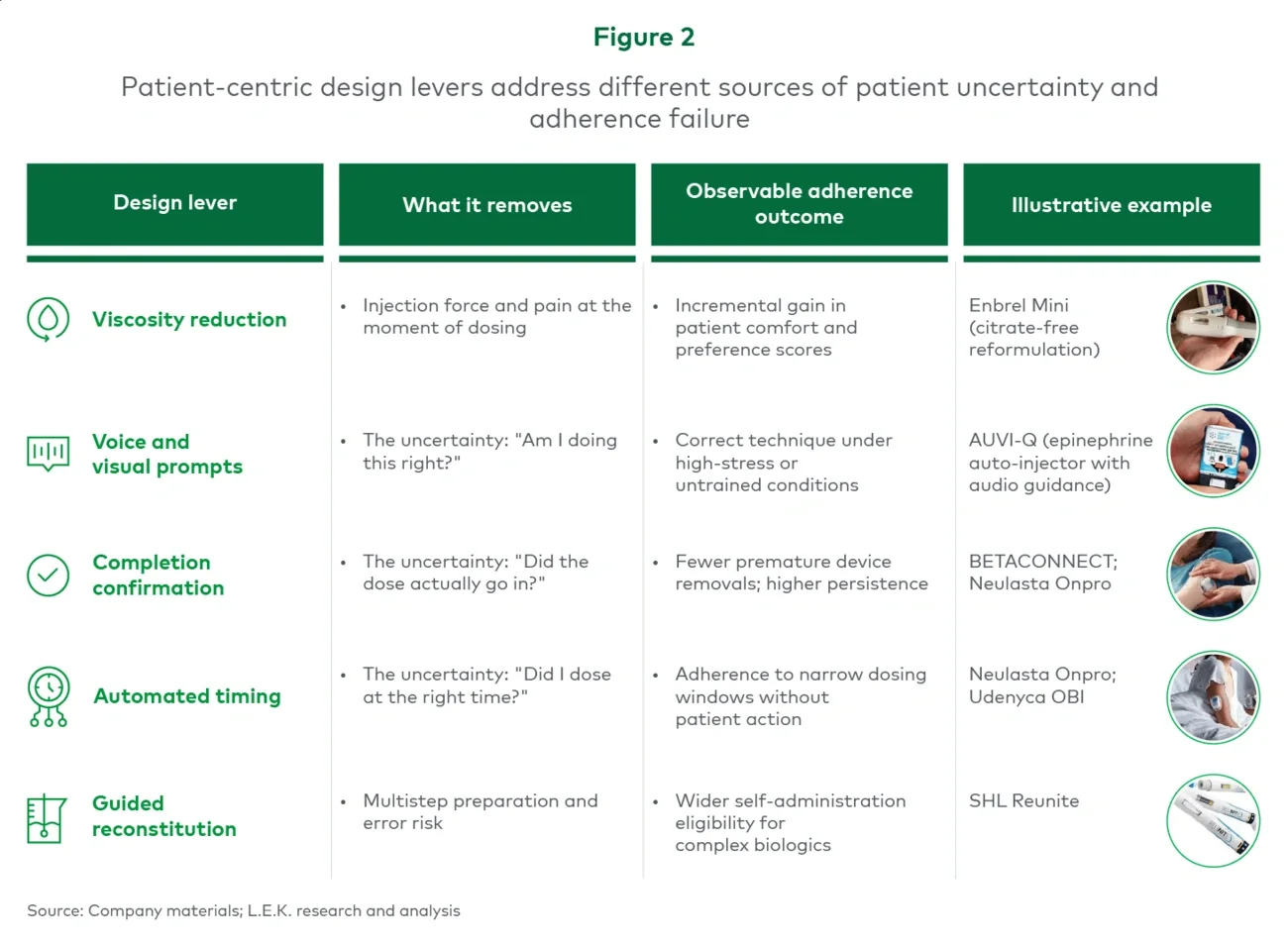
Three forms of uncertainty are particularly important:
- Am I doing this correctly?
- Did the full dose actually go in?
- Did I administer the dose at the right time?
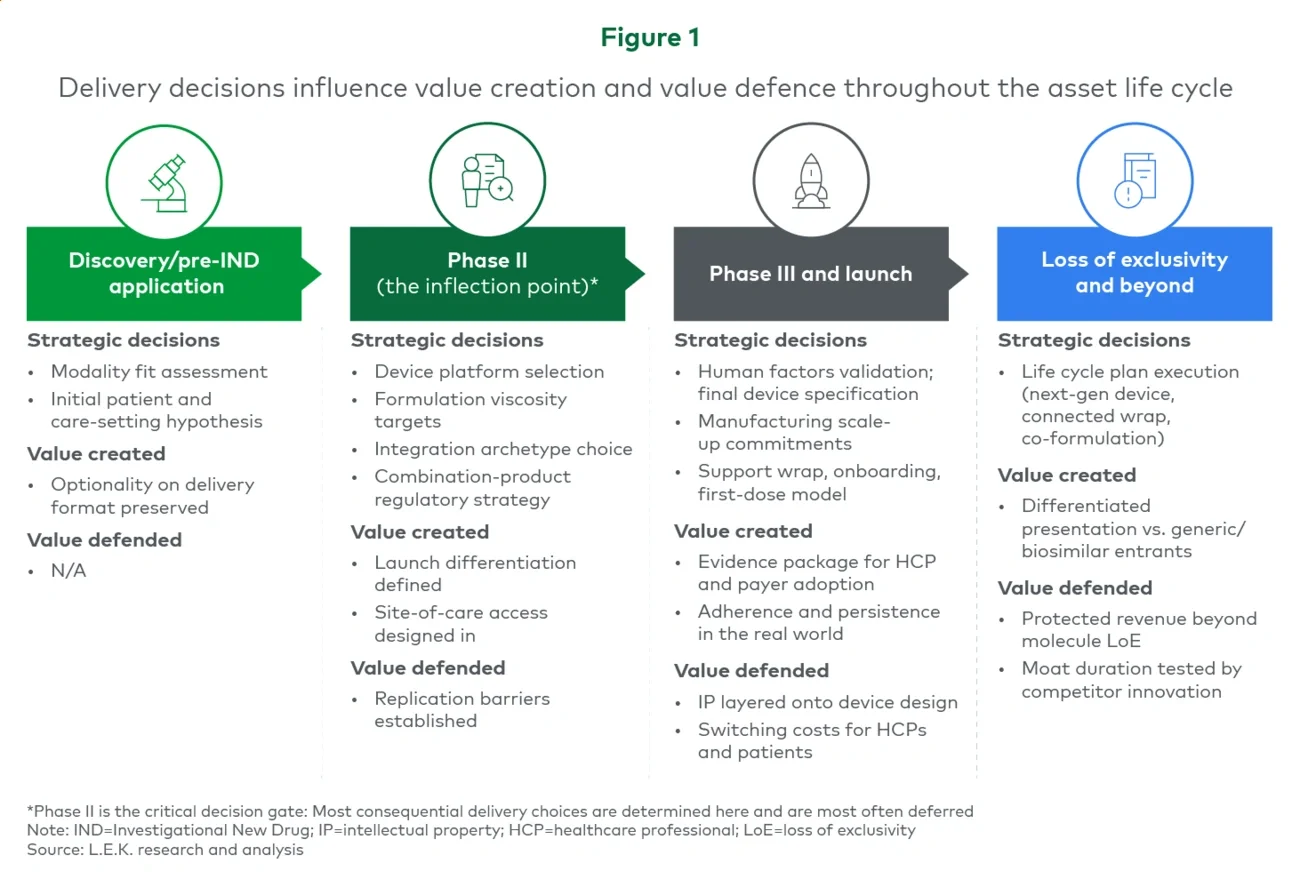
These uncertainties can emerge across the entire self-administration journey, from treatment preparation through to ongoing adherence (see Figure 1). Failure points are not confined to the moment of injection and often occur well before or after the dose is delivered.
The scale of this challenge is easy to underestimate. In one observational study of insulin injection technique among Canadian individuals with diabetes, every patient made at least one technique error, with the most common being incorrect applied injection force (76%), insufficient injection-site rotation (64%), insufficient needle dwell time (61%), incorrect reuse of needles (39%) and incorrect needle length (34%). These are not failures of willingness or comfort; they are failures of confident, correct execution that persist even in a mature, well-supported delivery category such as insulin.