Understanding changes to Medicare risk adjustment is paramount for payers and risk-bearing providers
The Centers for Medicare & Medicaid Services (CMS) originally introduced the CMS-HCC model in 2004 to better tailor Medicare capitation payments to managed care organizations based on expected beneficiary costs. The model assigns risk adjustment factors (RAFs) to hierarchical condition categories (HCCs) in order to predict a health plan’s cost of managing its specific population based on the relative complexity and burden of disease among its members.
Over the last 20 years, CMS has periodically updated the methodology to account for trends in underlying Medicare expenditure, evolving classifications of disease and Medicare budget considerations. Changes to the model are critically important to Medicare Advantage (MA) plans and risk-bearing providers that serve Medicare patients because they directly impact reimbursement.
This article evaluates the changes put forth in the 2024 CMS-HCC model (V28) and the implications for industry stakeholders.
V28 reduces the payment adjustment upside for sicker and more complex members
CMS finalized V28 of its risk adjustment model in 2023, with a glide path to full implementation taking place between 2024 and 2026. The new model delivers five key changes relative to the previous version:
- Switched from ICD-9 to ICD-10 codes: Despite the industry’s broader shift to ICD-10 codes, the CMS-HCC model had been using ICD-9 codes; V28 brought the model up to current industry standards by mapping diagnoses to ICD-10 codes, which should help drive standardization for data and reporting practices as well as greater specificity in capturing diagnoses.
- Updated fee-for-service base years: The new V28 model uses fee-for-service base data from 2018 (diagnoses) and 2019 (expenditures) to inform beneficiary trends and expected spend levels, aiming to further standardize payments between MA (typically higher) and Original Medicare.
- Increased number of HCCs but decreased relevant diagnoses: Under the CMS-HCC model, each HCC encapsulates multiple related ICD diagnosis codes; the V28 model increased the number of HCCs (from 86 to 115) but decreased the number of relevant ICD-10 codes by approximately 2,100 (from about 9,800 to roughly 7,700), meaning fewer diagnoses will drive RAF uplift in the new model.
- Reduced like-for-like RAF coefficients: Some HCCs received lower like-for-like RAF coefficients based on the updated base data, resulting in lower relative reimbursement.
- Introduced constraining coefficients: These “constraining coefficients” are intended to standardize RAFs for related diagnoses (e.g., the RAFs for the three different diabetes codes are equivalent in the new model, removing the additional compensation for diabetes when linked to other diagnoses).
Taken together, CMS expects the decrease in RAF scores to translate to about 3.12% lower payments and approximately $11 billion in savings in 2024. In the context of base rate cuts and broader headwinds in the MA segment, this new risk adjustment model further challenges profitability for MA plans and risk-based providers.
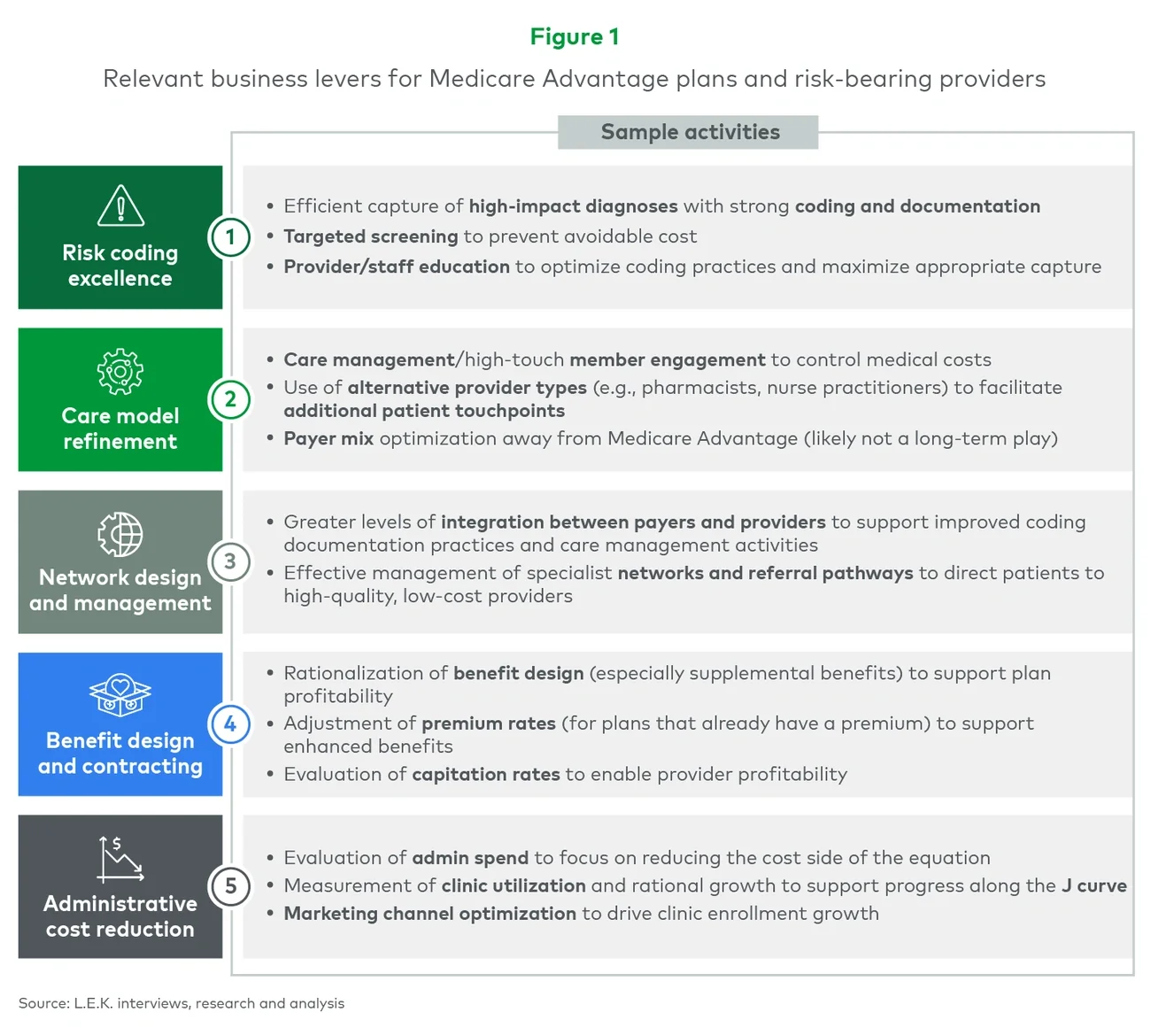
The V28 dynamic does not change the fundamental activities for MA plans and risk-bearing providers, but it does emphasize the importance of operational effectiveness to preserve margin
Insofar as the V28 model changes effectively bring a rate cut to MA plans and risk-bearing providers, they stress the importance of driving operational efficiency and business hygiene (see Figure 1).