For today’s health systems, patient access and system capacity are inseparable. The ability to meet community demand depends on getting both right. In L.E.K. Consulting’s 2025 Health System Executive Survey, more than 90% of U.S. executives said they face significant challenges on these fronts, from dropped referrals to workforce shortages.
These issues directly shape health systems’ growth and long-term resilience as well as the patient experience. In this edition of Executive Insights, we explore what executives tell us about the access and capacity challenges they are facing, the actions they are taking to address them and how leaders can better position their systems for sustained long-term growth.
The access challenge
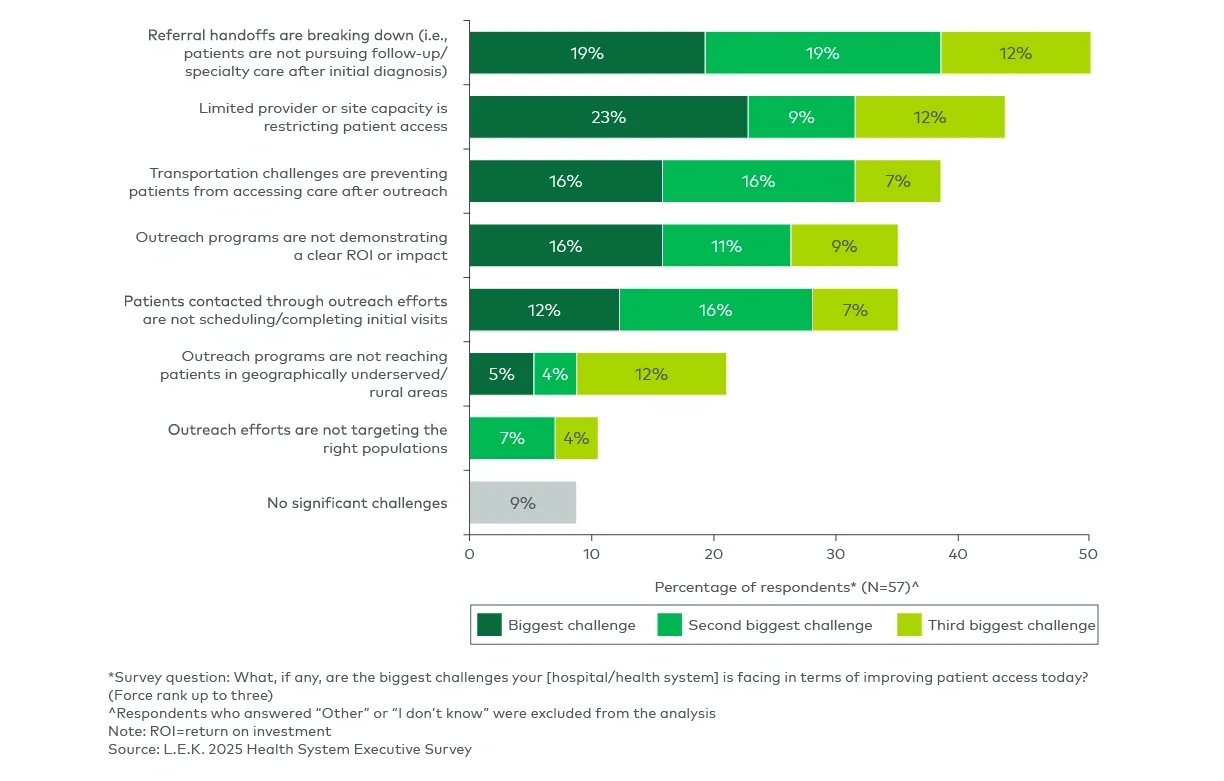
Access barriers continue to frustrate hospitals and health systems, with executives citing three as most pressing (see Figure 1):
- Breakdowns in referral handoffs: Patients often fail to pursue follow-up or specialty care after an initial diagnosis, leading to treatment gaps. These breakdowns reflect gaps in care coordination across providers and sites and highlight the lack of consistent navigation support once patients leave the initial care setting.
- Outreach effectiveness: Outreach programs frequently fail to demonstrate return on investment and often struggle with patient engagement, scheduling follow-through and addressing transportation barriers. This is particularly challenging in underserved communities where the need for access expansion is the greatest.
- System capacity limits: Leaders see provider and site capacity constraints as a critical barrier, because patient demand is met with scheduling delays that undermine timely access to care.