For behaviors that require persuasion through nuanced, individualized dialogue — such as deciding to prescribe a therapy with complex risk-benefit trade-offs — personal promotion is the anchor. A live conversation with a medical science liaison (MSL) can surface concerns no digital banner could. Even so, nonpersonal tools — like a short explainer video, follow-up text or concise evidence digest — help educate prior to making a decision and reinforce the exchange after a decision has been made.
When the barrier to the behavior change stems from a straightforward information gap, recognition lapse or procedural misstep, scaled digital tactics focused on educating, enabling and/or reminding can shoulder more of the load. Take physician office activation for prior authorization as an example: Interactive microlearning modules, autopopulated checklists in the electronic medical record (EMR) system and real-time status alerts can standardize submissions and cut cycle time. A field reimbursement manager remains on call for escalations, providing a targeted human touch when digital alone is not enough.
Personal engagement: Design the customer-facing model
Delivering the personal side of engagement requires a clear customer-facing model with a blueprint for which roles engage which stakeholders and how those interactions are coordinated.
Certain roles — sales representatives, MSLs and national account managers — form the backbone of nearly every launch. During go-to-market planning, companies must decide which additional roles to layer on and at what scale.
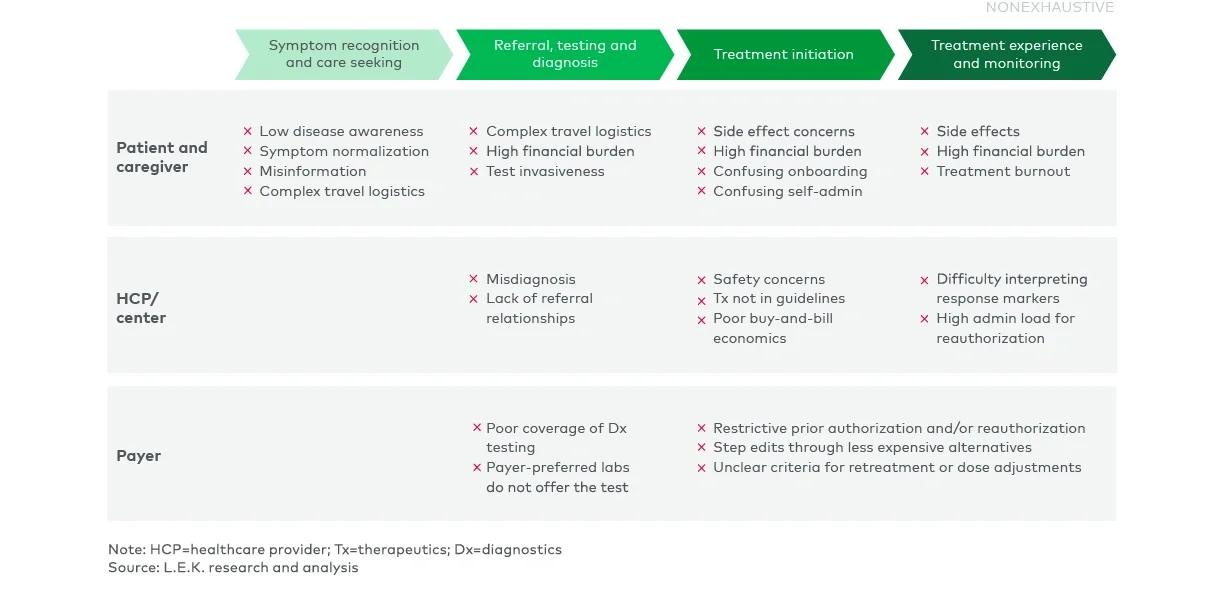
This should be dictated by the behaviors the company has prioritized and the skills required to shift them. If diagnostic inertia is a constraint, deploy diagnostic specialists who can walk clinicians through test-ordering workflows. If access friction is resulting in patient drop-off, plan for a robust field reimbursement manager force to navigate prior authorization appeals and benefit investigations. When administration is complex, nurse educators equipped to train infusion sites and coach patients become critical.
Equally important, coordinate these specialists’ outreach so stakeholders experience a seamless dialogue — not a barrage of overlapping touchpoints.
The customer-facing model assigns the right roles to the right behaviors, maintains the necessary share of voice and reserves human expertise for the moments when personal engagement drives outcomes.
Deploy nonpersonal engagement
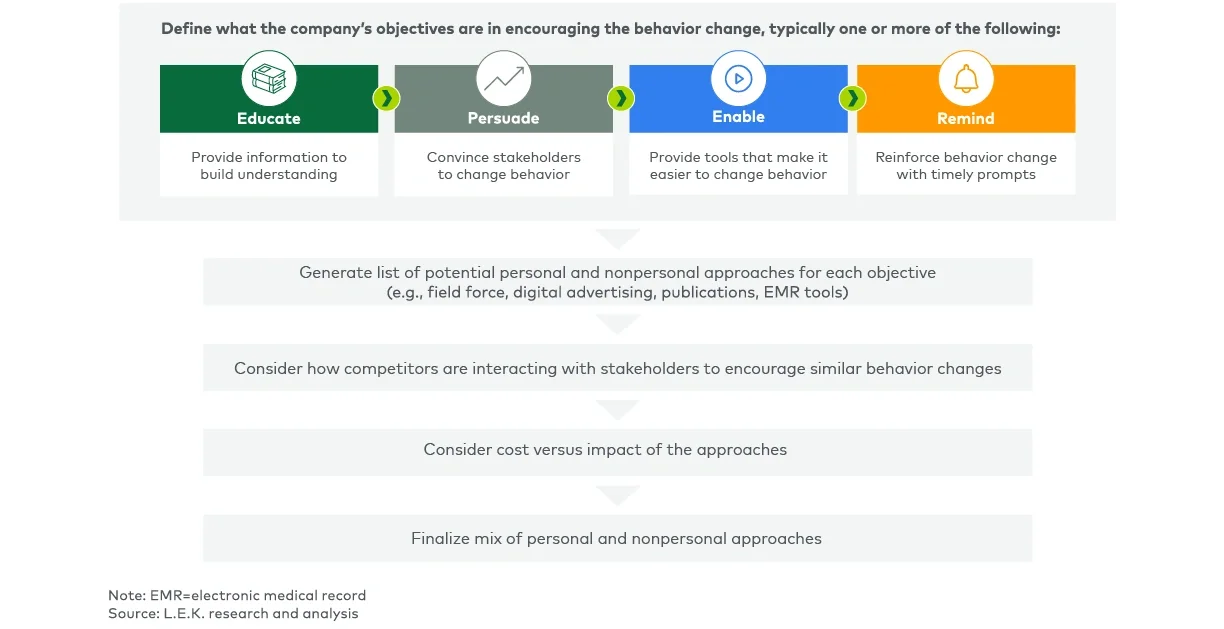
Nonpersonal engagement is also critical for behavior change and demands the same disciplined planning as personal engagement. At the go-to-market strategy stage, the goal is to match each prioritized behavior with the nonpersonal approaches most likely to shift it, gauge the investment those approaches will require and surface net new capabilities — such as EMR system integration or modular content operations — so budgets and roadmaps are grounded before detailed tactical planning begins.
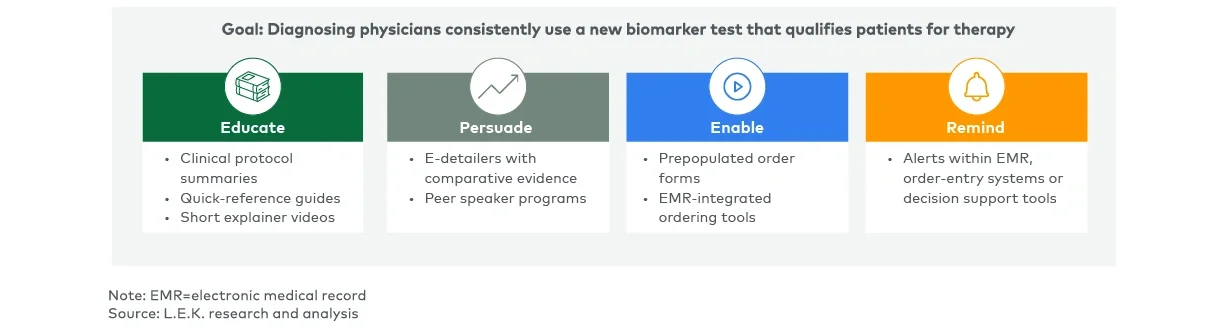
The most effective programs anchor nonpersonal engagement in the behavior that needs to shift and what it will take to make that happen. Take the example of slow adoption of a new biomarker test despite guideline inclusion, where nonpersonal engagement approaches are coordinated to collectively educate HCPs about the biomarker test, persuade them of the benefits of using it, enable them to easily order it and remind them on an ongoing basis when patients are appropriate for that test (see Figure 4).