While funding and dealmaking trends underscore a growing resurgence, committed neuroscience players are still mindful of the therapeutic area’s inherent risk and volatility. Some are complementing their neuroscience pipelines with assets in other disease areas to balance risk. For example, Acadia Pharmaceuticals has expanded into rare disease with their Rett syndrome therapy Daybue and are building on this momentum with pipeline therapies in Prader-Willi and Fragile X syndromes.
Similarly, Biogen continues to invest in Alzheimer’s and ALS while advancing late-stage systemic lupus erythematosus assets as part of a growing immunology presence. These strategies highlight that even among a scientific renaissance in neuroscience, long-term success may depend on pairing innovation in this area with a diversified portfolio.
Areas for Continued Investment
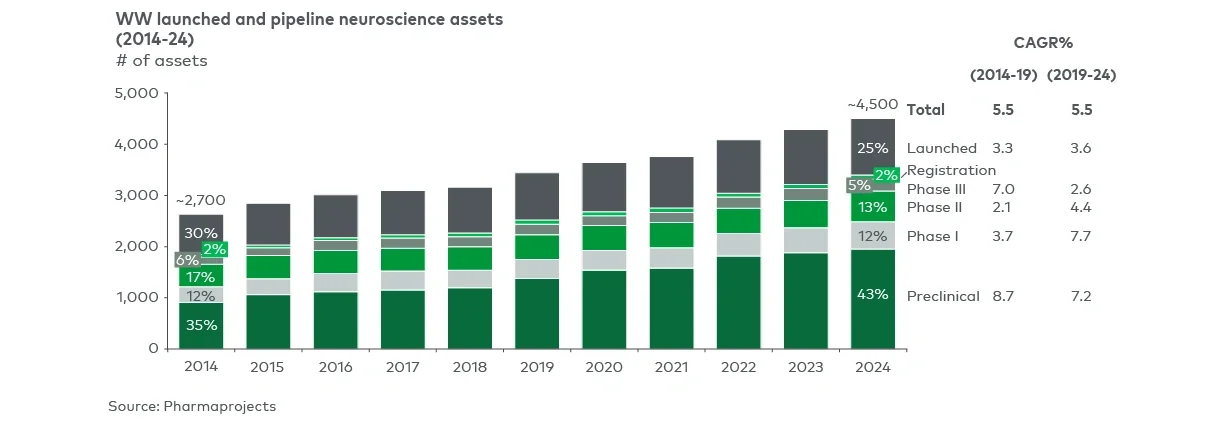
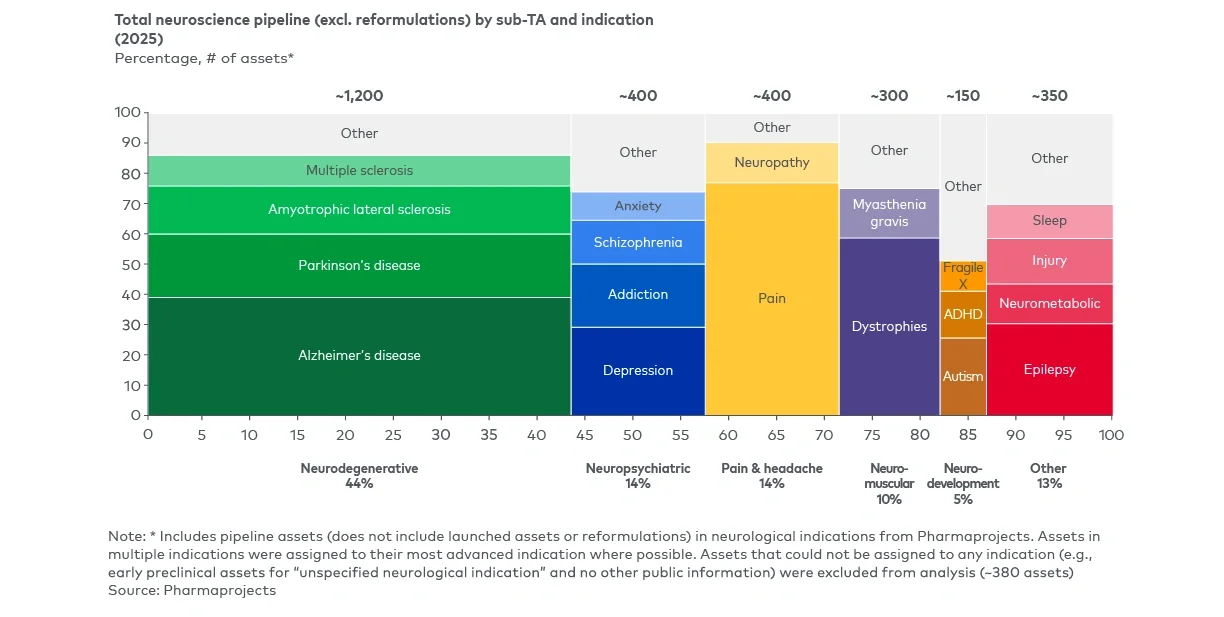
Despite recent progress, significant unmet needs persist across various areas within neuroscience, particularly in neuropsychiatric, pain, neurodevelopmental, neuromuscular, and neurodegenerative conditions – fueling total pipeline activity (see Figure 6). Looking ahead, promising avenues for innovation and investment are emerging, including:
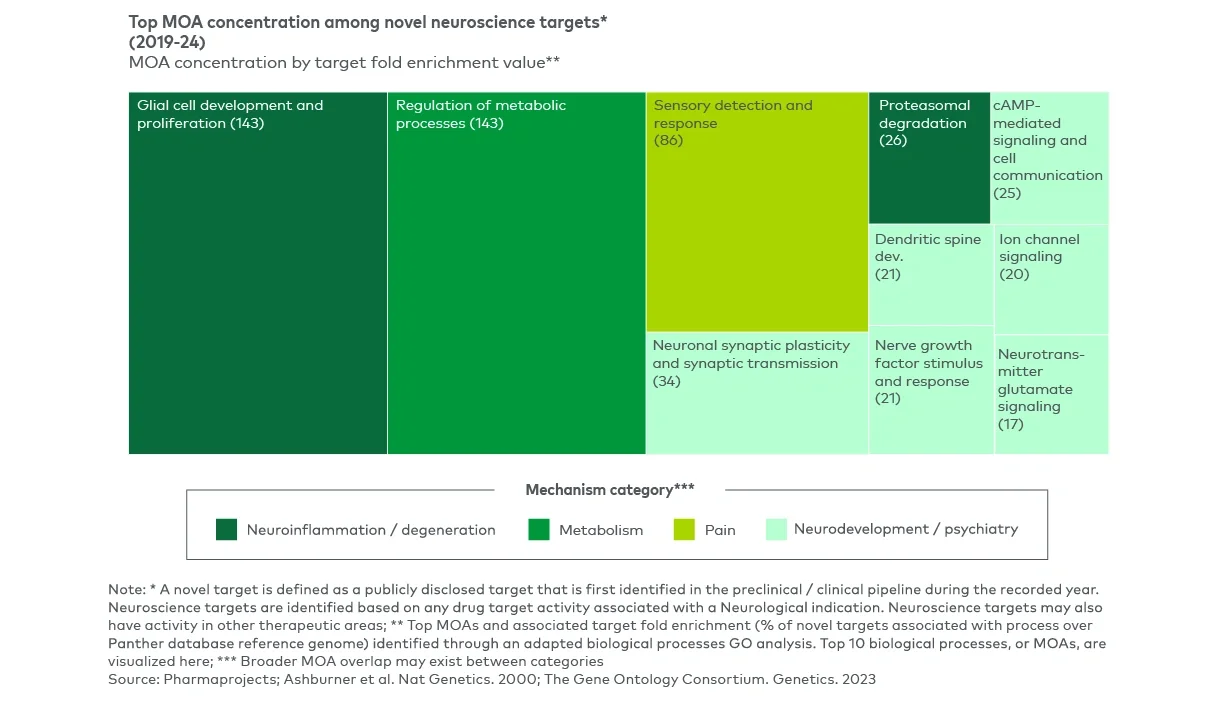
- Developing new approaches to validated pathways, including through the adaptation of learnings in other therapeutic areas (such as leveraging immunology targets within neuroscience indications)
- Exploring complementary disease mechanisms within attractive pathways, including the use of polypharmacy or combination regimens that engage multiple MOAs, whether within the same pathway or across converging biological axes
- Investigating new modality/delivery approaches to expand on the types of targeted therapies that can be utilized within the CNS
- Leveraging enabling technologies to enhance drug development, support patient identification, and improve clinical outcome measurements
In neuropsychiatric disorders, including treatment-resistant depression, addiction, and schizophrenia, emerging treatments such as NMDA modulators and psychedelic-based therapies build on established areas of excitement but require further clinical validation. Additionally, approvals and clinical activity against first-in-class M1 and M4 muscarinic targets (e.g., Cobenfy, Emraclidine) expand beyond established approaches to target dopamine-specific pathways for antipsychotic treatments. Meanwhile, advances in functional imaging and digital phenotyping (e.g., Alto Neuroscience’s Precision Psychiatry Platform) are supporting more targeted and biomarker-guided approaches to clinical development.
Similarly in pain indications, the focus has been on developing novel, non-opioid targeting treatment to move beyond historic strategies for chronic or severe pain management. Attractive mechanisms being pursued today include identifying how targeting different sensory pathways , such as itch, can help alleviate conditions of pain. Recent advancements into new targeted therapies include Vertex’s Journavx, a first-in-class non-opioid treatment (targeting NaV1.8) for patients with moderate-to-severe acute pain. Additionally, Kriya Therapeutics recently raised over $300M to advance its pipeline of gene therapies, including a program targeting trigeminal neuralgia, further illustrating how diverse modalities are now being applied to historically underserved pain conditions.
Neurodevelopmental and neuromuscular disorders, especially rare genetic conditions such as Duchenne muscular dystrophy (DMD), present both technical challenges and opportunities for modality innovation. For example, in DMD, the development of gene therapies has been complicated by the size and complexity of the DMD dystrophin gene and safety concerns regarding gene therapy use. Sarepta’s Elevidys has faced a series of clinical and commercial setbacks, but newer micro-dystrophin constructs utilizing different AAV vectors are in development and have the potential to offset both efficacy limitations and the safety concerns seen with Elevidys.
Alternative marketed strategies exist to target the DMD gene mutations (e.g., exon-skipping ASO therapies) but have yet to achieve sufficient efficacy, partly due to limitations in tissue targeting. However, companies are currently working to develop more targeted therapies that can improve on current safety and efficacy standards. For example, Avidity is developing a next-generation exon skipper designed to better target muscle cells by utilizing an antibody-oligonucleotide conjugate to increase tissue specificity.
In neurodegenerative diseases, inflammation-targeted therapies are gaining attention as potential disease-modifying treatments. In ALS, therapeutic progress has been difficult due to disease heterogeneity and rapid progression, as underscored by the recent withdrawal of Amylyx’s Relyvrio. However, pipeline candidates are exploring upstream mechanisms like TDP-43, mitophagy and axonal transport, and are directly targeting inflammatory signaling as in RAPA-501, an autologous T-cell therapy that enhances regulatory immune function. These programs represent a multimodal strategy tailored to a disease landscape where heterogeneity limits the likelihood of a single, uniform solution.
In Alzheimer’s disease, R&D activities have expanded beyond the classic hallmarks of amyloid beta and phosphorylated tau to include additional targets such as glial-neuronal cross-talk, oxidative stress and proteostasis. In parallel, developers are innovating on existing amyloid approaches with subcutaneous or oral delivery forms (e.g., Eli Lilly’s remternetug, Annovis’s buntanetap), improved blood-brain barrier delivery (e.g., Roche’s blood-brain barrier shuttle), and combination trials investigating multi-target approaches, which are gaining traction as understanding of disease biology broadens.
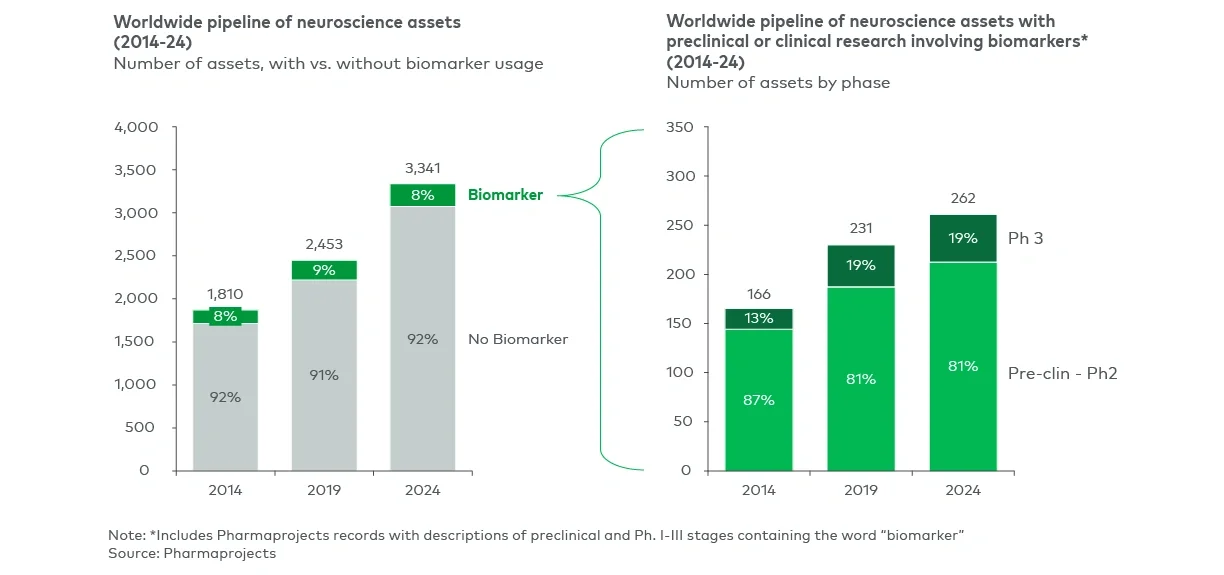
Alongside innovation in MOAs and delivery technology, biomarker development is expanding to include blood-based, imaging-based and digital tools; for example, Johnson & Johnson is investigating ways to use machine learning to measure changes in speech patterns that may be predictive of early Alzheimer’s. These approaches reflect the continued centrality of amyloid and tau, complemented by a broader, multi-pathway understanding of disease biology and the technologies needed to target mutation more effectively as well as identify it earlier in the disease course.