Radiolabelling at the core of CDMO offerings
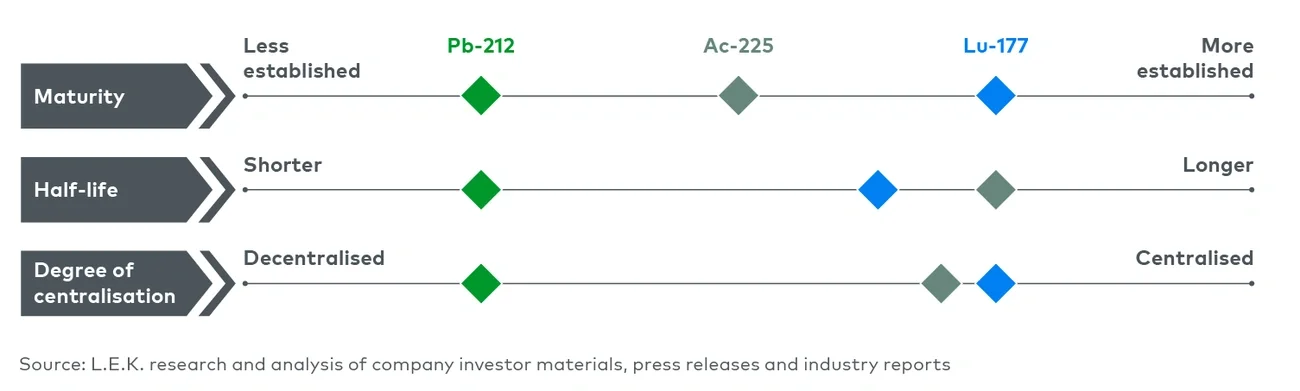
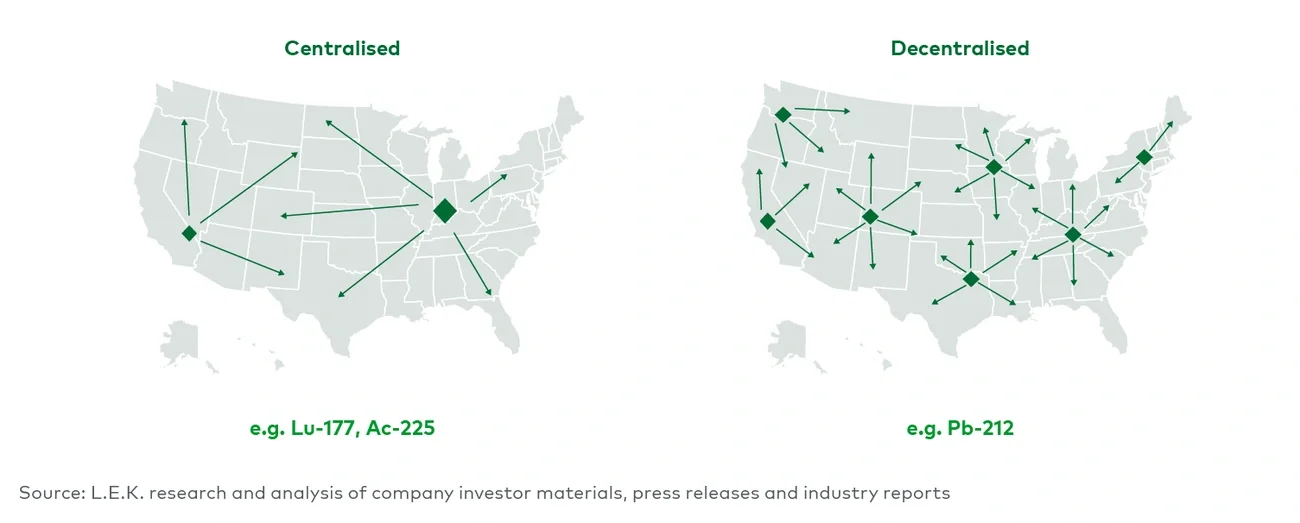
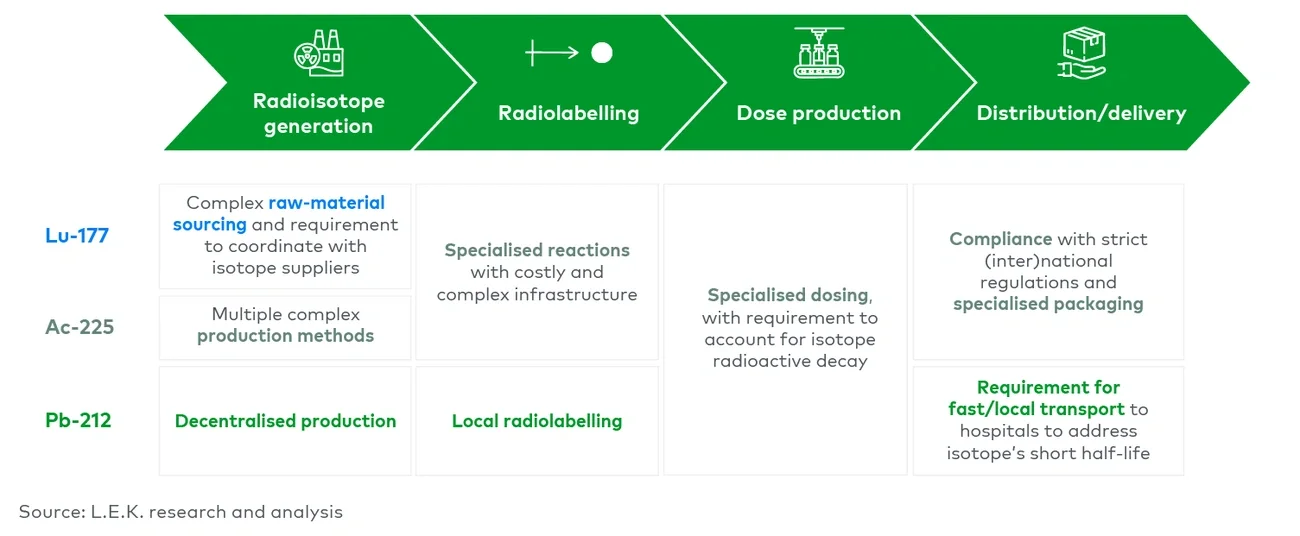
Subsequent radiolabelling connects the radioisotope to the targeting ligand via chelation. For Lu-117 and Ac-225, radiolabelling can be performed in centralised facilities owing to their relatively long half-lives. The specific conditions vary based on chelator and isotope, but labelling may require high temperature and pressure requirements alongside radioactive compound handling precautions.
Whilst biopharma may want to consider in-house labelling for supply security and quality control, CDMOs can play a key role to avoid costly investment as well as complexity in infrastructure (e.g. shielded laboratories, handling systems such as hot cells, glove boxes) and procedures for biopharma. CDMOs can also bring substantial expertise in chelation and ultimate linking of targeting compound and radioisotope that are difficult to establish for new entrants (see Figure 4). Example CDMOs currently in the field include SpectronRx and NorthStar.
Pb-212’s shorter half-life necessitates local radiolabelling and therefore a more widespread geographical footprint. CDMOs can play a key role in accommodating local needs for radiolabelling due to the isotope’s shorter half-life.
More broadly, radioactive decay drives the need for radiopharma CDMOs to more frequently produce (smaller) batches throughout the year in contrast to the potential for larger, more infrequent batch sizes for other therapeutic modalities. The more continuous nature of production drives higher utilisation rates, which could lead to different operations and levels of profitability when compared to other therapeutic-modality CDMOs.
Extending CDMO capabilities into dose formulation and logistics
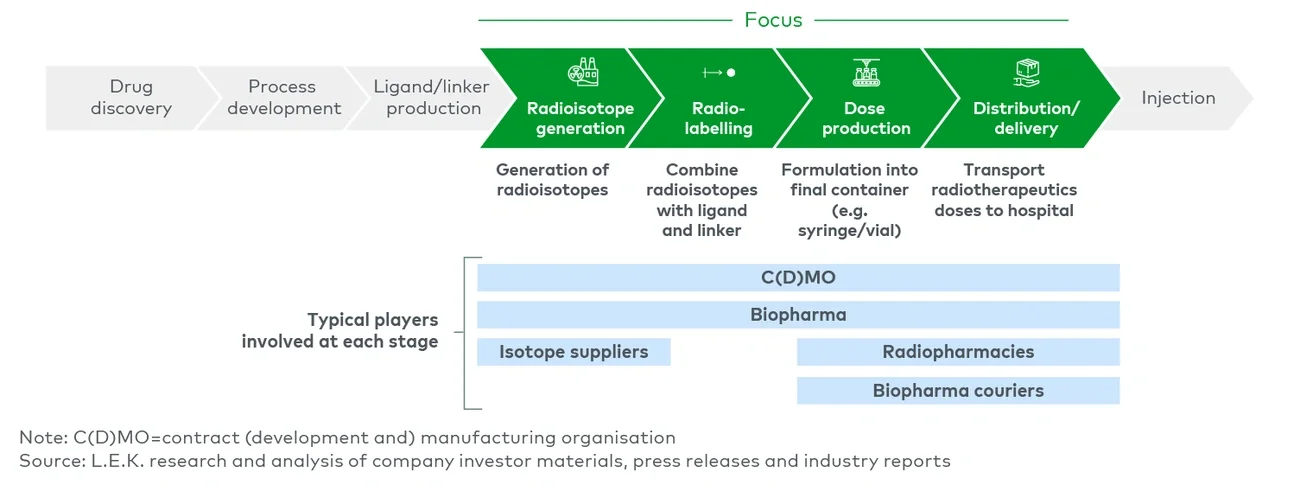
Following radiolabelling, the compound is formulated into ready-to-administer syringes or vials. This stage is specialised, as the therapeutic dose needs to be accurately measured to maximise efficacy while minimising toxicity. Dosing is complicated by the radioactive decay of isotopes, which must be accounted for in the production process to ensure that patients receive the intended radiation dose.
CDMOs can oversee this process for companies without in-house capabilities. Radiopharmacies are another player that can perform this step, though some facilities operate as both a CDMO and a radiopharmacy.
Distribution and delivery represent the final step prior to patient administration. Due to radioisotope decay, this process must be carefully managed. Shipping requires compliance with strict (inter)national regulations, and specialised packaging is essential to ensure safety during transport. Depending on the isotope and capabilities of the players in the value chain, there could be anywhere between one and three players exchanging radioactive intermediates or final dose product prior to final delivery for patient administration.
The short-half-life of the radioisotope is a key parameter to consider for logistics and reinforces the importance of integrated providers, as evidenced by Orano Med’s specialised logistics for Pb-212. In North America, for example, Orano Med’s ATLab, leveraged for large-scale production, is strategically located in Indiana next to major national and international distribution hubs and delivery companies (e.g. FedEx) to ensure fast transport to hospitals and address the 10.6-hour half-life of the isotope.
Challenges in this step may result in potential for more biopharma courier services to expand their offering into radiotherapeutics and leverage the optimisation and speed of their logistics. Companies such as Life Couriers provide logistics services for radiopharmaceuticals and may also cover other sensitive biopharma products, such as live cells, as adjacent services. Once the radioisotope is received, hospitals and treatment centres play a critical role in final correct handling, storage and patient administration.