What are the causes, and what can be done?
Issues with diagnostic approach: The existing diagnostic paradigm for psychiatric disorders, such as the DSM-5, inadequately considers the cultural nuances that significantly influence the clinical manifestation of psychopathology in individuals of colour. For example, the current diagnostic criteria for PTSD do not include race-based trauma. Without these culturally inclusive diagnostic criteria, minorities often do not qualify for treatment studies, reducing their overall representation relative to the general population in some studies.
Unlike in many other psychiatric drug trial designs, researchers in psychedelic studies have not accounted for this inherent bias and thus far have been unable to recruit participant groups that represent greater ethnic diversity.
Ineffective and narrow recruitment methods: Many trial participants are referred from outpatient providers, including physicians and mental health clinicians. These centres typically treat a lower proportion of patients from diverse ethnic backgrounds, as certain factors – e.g., cultural and social stigma regarding seeking medical help, the cost of physician fees – might prevent individuals in marginalised groups from reaching care.
If researchers in psychedelic trials sought referrals from providers that accept Medicaid and other forms of affordable healthcare in the US, they would likely experience greater success in recruiting minority ethnic groups.5 Researchers with specific expertise in areas of cultural diversity and the recruitment of people of colour should be included in trial teams, and efforts should be made to recruit more researchers from minority groups into the psychedelic field.
Increasing the diversity of therapists involved in clinical trials would improve participant recruitment as well as the research itself. Sunstone Therapies, based in Rockville, Maryland, US, is a leading clinical trial centre for psychedelic-assisted therapy in the medical setting, and keen to promote more diverse therapist populations. Manish Agrawal MD, Chief Executive Officer at Sunstone Therapies, says: “Having clear sightlines for understanding perspectives, and investing in diversity, equity and inclusion for therapists, is crucial to the overall health and foundation of research into psychedelic-assisted therapies. We have funded a project with Dana-Farber to identify and understand the opportunities and barriers for Black therapists to engage in this field. We need more initiatives like this across the industry so that we develop culturally informed research designs, training programs and funding opportunities – and can accelerate the diversification and equity of psychedelic research.”
Insufficient incentivisation to overcome hurdles: Many recent psychedelic studies in the US have been privately funded, which means they were not required to conform to National Institutes of Health (NIH) diversity guidelines. The NIH Revitalisation Act of 1993 mandated that all studies supported by NIH funding must carefully consider the proportions of ethnic minorities and women in a study population, ensuring representative numbers compared with the overall population.6 However, in the UK, the Health Research Authority (HRA) has been working with groups of researchers, public contributors and research ethics committees to develop supporting guidance for researchers to consider when designing clinical trials, so that they develop a better understanding of the most effective treatments for different groups of people.
As government funding and focus increase, further emphasis on recruitment criteria and appropriate demographic representation is anticipated.
Sex and gender diversity
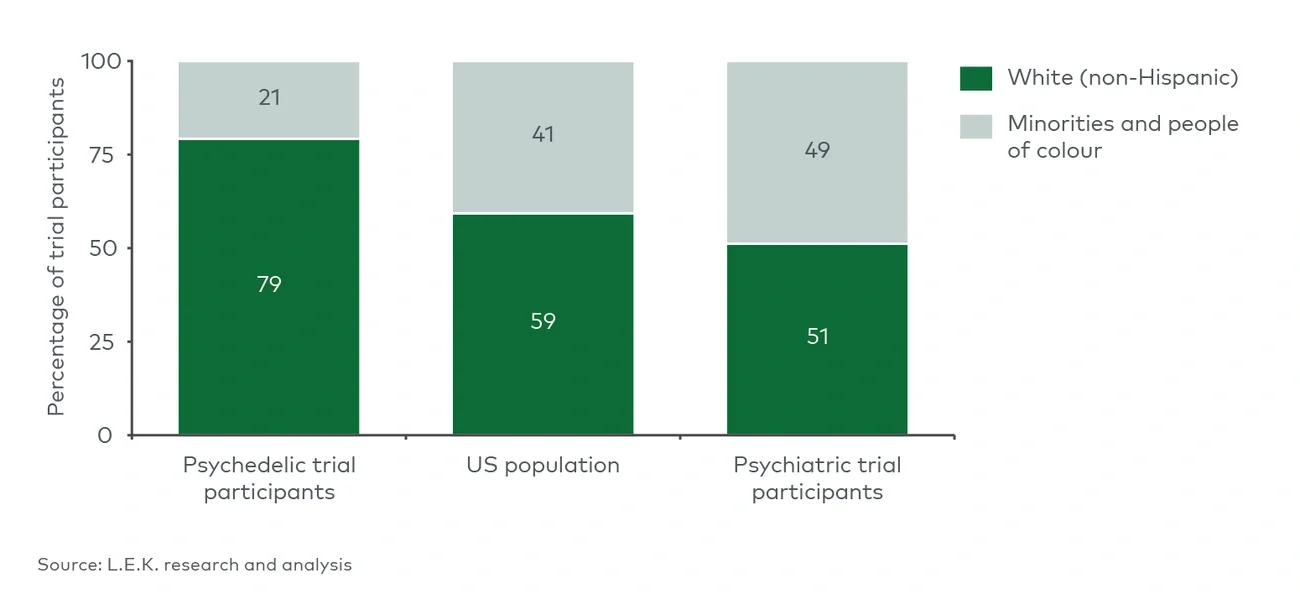
From a gender perspective, trial recruitment has historically been more balanced. Of the 20 psychedelic studies whose demographics were analysed, 58% of the trial participants were female, and the most recent MDMA study contained more females in its sample than males, accurately representing the demographics of the PTSD patient pool.7 Greater female representation in clinical trials will support increased confidence in the safety profile for women, an issue that has historically arisen in trials with disproportionately low female representation.8
However, the historical underrepresentation persists in PTSD research, for example, of transgender and gender-diverse people, who experience trauma and PTSD at higher rates than the general population.9 Including gender-diverse participants in such studies is important for understanding the efficacy of psychedelic therapies for those suffering from gender-based trauma.
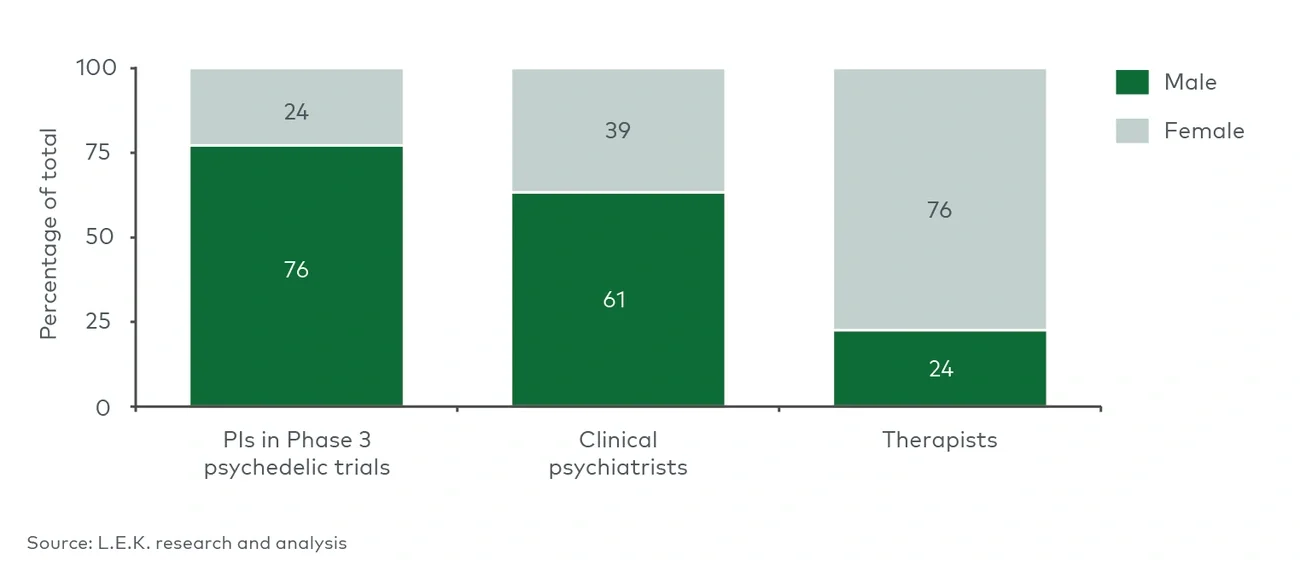
The issue relating to gender extends beyond the recruitment of trial participants and lies more fundamentally in the people leading the psychedelic movement in psychiatry. Of the 46 principal investigators leading Phase 3 psychedelic clinical trials, 76% are male and 24% are female. Unfortunately, this type of imbalance is common across many scientific research fields. When compared with the percentage of female clinical psychiatrists in the US overall, the psychedelic field comes up short once again (see Figure 4). The disparity is even greater when comparing the trial investigators to the number of therapists in the US, where 76% are female. Addressing this disparity will likely facilitate a more balanced interpretation of clinical results, ensuring they are more applicable to the wider population.10