One example is a hospital network that has rapidly expanded by catering almost exclusively to BPJS patients. This network of hospitals has positioned itself as a “BPJS-focused,
high-volume” provider. By locating hospitals in second-tier cities and peri-urban areas, it taps pent-up local demand where public facilities are scant and few private competitors operate. These hospitals recruit younger doctors and clinicians who are keen to build their careers. Doctors follow structured clinical protocols set by the network — ensuring that care delivery is standardized and efficient, rather than dependent on individual doctor preferences. This approach increases throughput (more patients treated per doctor)
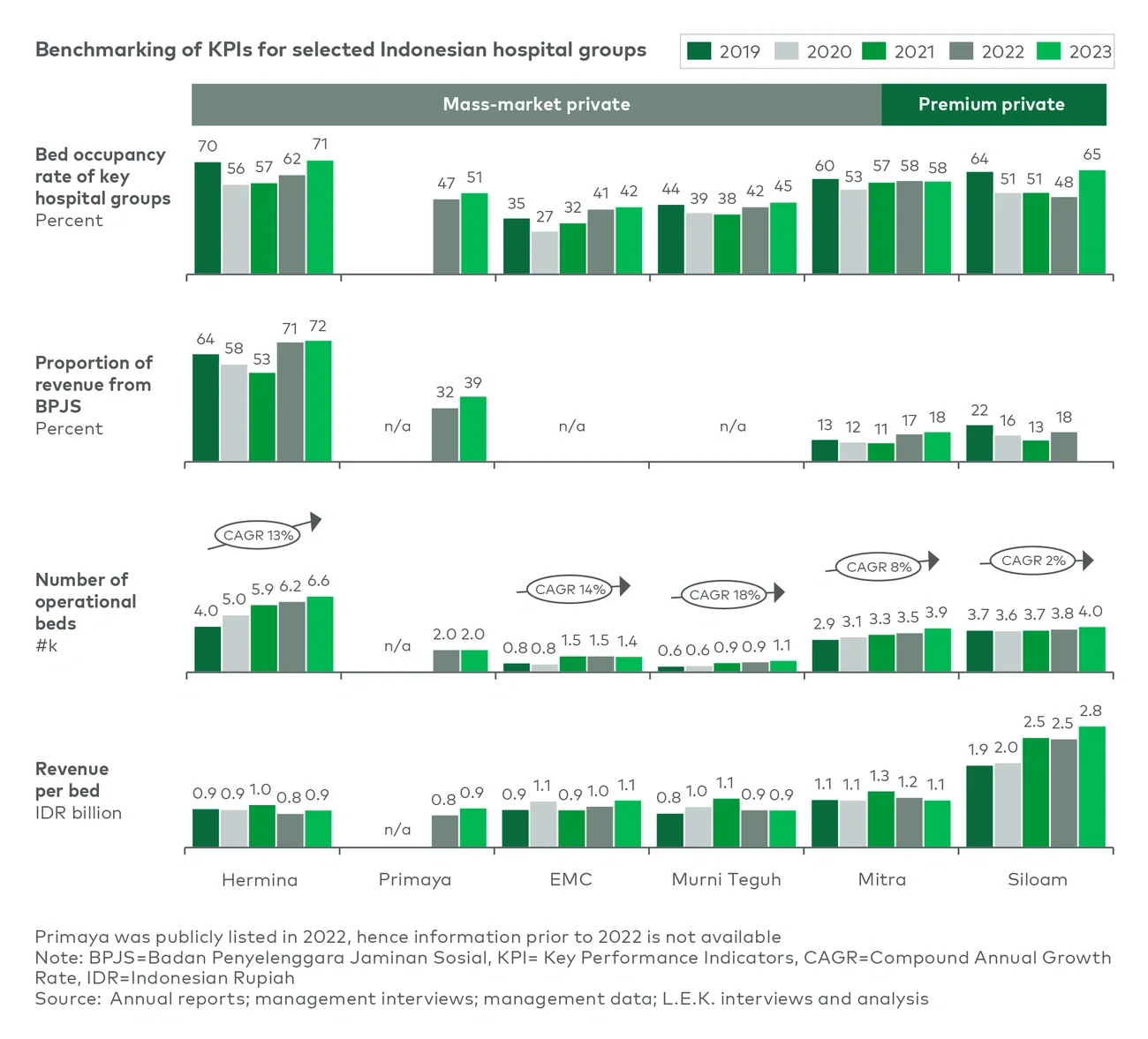
and aligns with BPJS guidelines for appropriate care. Importantly, the network exercises strict cost discipline in all aspects: from bulk procurement of generic drugs and supplies to lean hospital administrative staffing and utilitarian facilities. The result is a sustainable economic model even at BPJS’s modest tariff levels. High bed occupancy and volume drive revenue, while low cost per patient preserves a reasonable margin. This mass-market strategy can succeed where a traditional private hospital might fail. As evidence, some of these value-focused hospitals are reportedly profitable, with EBITDA margins in the high teens and above, despite 70%-80% of their patients being JKN-funded.5 They demonstrate that with the right scale and rigor, serving the masses is not just a social mission but also a viable business.
Indonesia’s government insurance administrators have indirectly encouraged such private participation by maintaining JKN financial stability in recent years. Moreover, the sheer volume growth of insured patients (tens of millions added in the past few years) means that even at low unit prices, the revenue pool is expanding. In summary, Indonesia’s mass- market hospital opportunity hinges on executing a disciplined, volume-driven model. Those who can streamline operations and work with government payers are poised to capture a huge share of Indonesia’s healthcare growth story, all while delivering accessible care to communities that need it most.
Premium players: Investing in advanced care
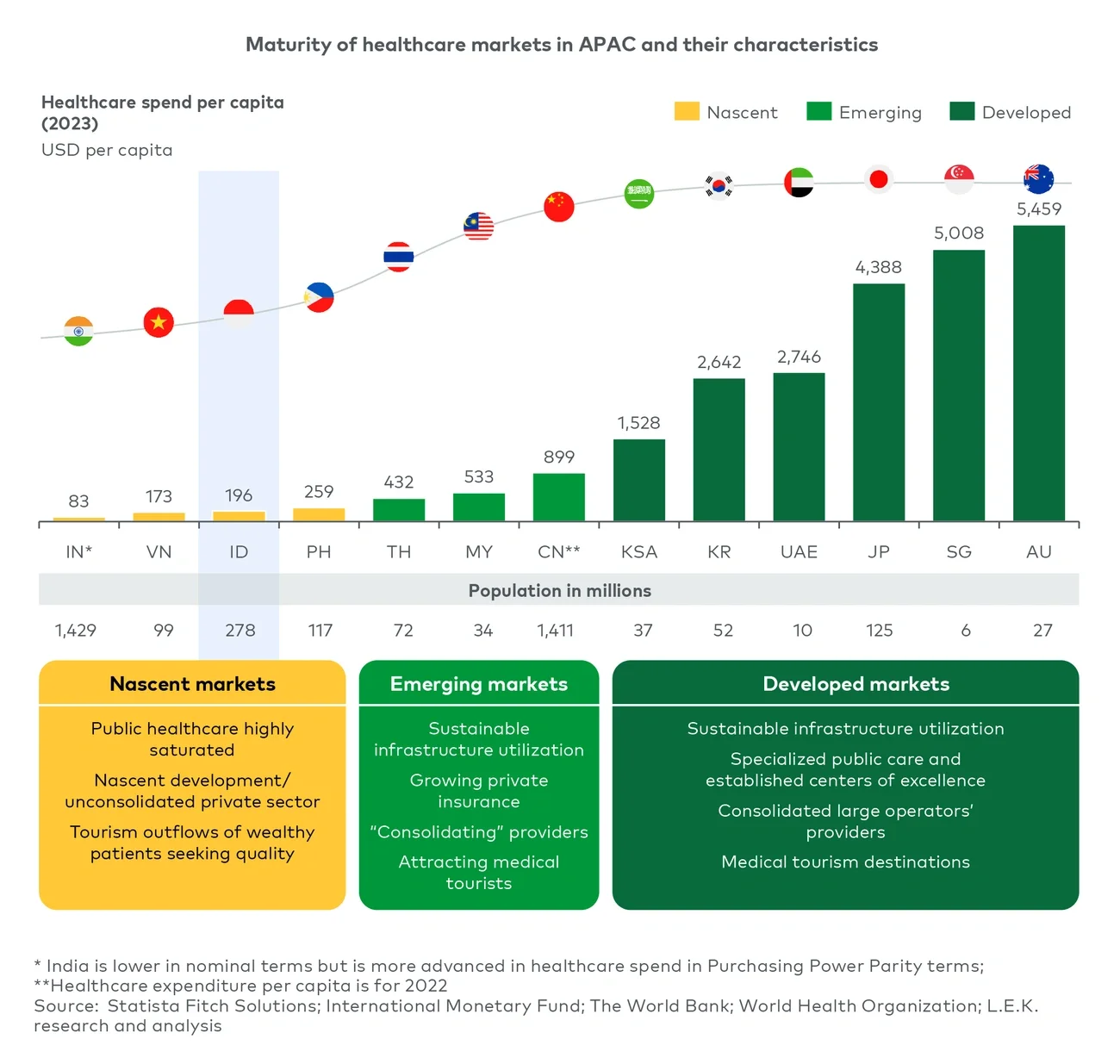
Even as mass-market providers race to add basic capacity, Indonesia’s premium hospital segment is also gaining momentum. In major urban centers like Jakarta, Surabaya and Bandung, several private hospital groups are positioning themselves to capture demand for complex and specialized care that historically was met through outbound medical tourism. (In nascent markets, wealthy Indonesians have often traveled to Singapore, Malaysia or beyond for advanced treatments — but this dynamic is beginning to change.) The leading private hospital players in Indonesia are now making significant investments in cutting- edge medical technology and specialty services to keep affluent patients in the country.
A clear example is oncology. Indonesia has a high and growing cancer burden, yet access to advanced cancer treatment has been limited domestically — for instance, there are only a handful of linear accelerators (LINACs) for radiotherapy in the entire country. Recognizing the gap, some private groups are stepping up. One major hospital network in Jakarta is in the process of installing Indonesia’s first proton therapy center, an advanced form of radiation therapy, as part of an expansion that includes six new hospitals by 2027.6 This multimillion-dollar investment signals confidence that demand for high-end oncology services will rise and that patients will pay for quality care at home rather than flying to Singapore or the United States. Likewise, several hospitals have recently acquired or are planning to acquire LINAC machines for conventional radiotherapy — often holding off only until they see sufficient private-pay patient volume to justify the expense. Currently a large portion of Indonesian cancer patients either rely on overcrowded public facilities or go abroad, so private hospitals see an opportunity to repatriate that volume by offering comparable technology.
Cardiac care is another area of focus. Many premium Indonesian hospitals are equipping cardiac catheterization labs (for angioplasty, stenting, etc.) and establishing heart centers, as heart disease remains the country’s top killer. The leading hospitals accredited by Joint Commission International in Jakarta now each boast multiple catheterization labs and cardiothoracic surgery teams and are starting to perform complex interventions that were rarely done in-country a decade ago.7 Investments in high-end diagnostic imaging are also evident — for example, 3.0 Tesla MRI machines and 256-slice computerized tomography scanners (the latest generation) are now present in several private facilities, matching the technology offerings of Singapore’s hospitals.8 Across the board, centers of excellence are being developed: from neurosciences units with advanced MRI and stroke care, to in vitro fertilization (IVF) clinics targeting Indonesia’s growing IVF market. These moves not only attract patients who would otherwise go abroad but also help capture the growing expatriate community and medical tourism inflows from neighboring countries (e.g., patients from East Timor or Papua New Guinea coming to Indonesian hospitals).
For investors specifically eyeing the premium hospital space, Indonesia offers a chance to ride an upgrade cycle. As the country’s healthcare system matures, what is considered “premium” today (e.g., basic cardiac surgery or simple cancer care) will become more commonplace, and truly advanced offerings (organ transplants, gene therapy, etc.) will define the new premium. The current wave of capital expenditure on proton therapy, LINACs, robotic surgery systems and other high-end equipment is laying the groundwork for Indonesia’s private hospitals to become regional leaders in care quality. Within a decade, Indonesia could conceivably retain a significant portion of its outbound medical tourism flows — especially if costs undercut Singapore or U.S. prices. The investor thesis here is to back those groups that are investing wisely in technology and talent, creating high barriers to entry and strong brand equity for top-notch care. So far, early adopters are already seeing returns: Many premium hospitals report healthy growth in revenue per patient. With the government’s tacit support (e.g., special economic zones such as Bali and Batam,9,10 or allowing foreign specialist hiring in limited cases), the premium segment is set to flourish alongside the mass-market boom.
Policy tailwinds: Government commitment and reforms
The Indonesian government has explicitly linked healthcare improvement to its broader national development agenda. President Joko Widodo’s administration articulated the vision of a Golden Indonesia 2045, wherein Indonesia achieves high-income status by its centenary. A key pillar of this vision is a healthier, more productive population — which implies reducing premature mortality and boosting human capital. To address systemic challenges and unlock the full potential of its healthcare system, Indonesia is pursuing reform on three key fronts.
1. Targeting high-mortality diseases through preventive care
A country cannot become fully developed if a large portion of its people die in their prime or suffer chronic illness. To have an educated, productive workforce in 2045, the parents of those workers should not die prematurely; if they do, families fall into hardship and the next generation’s education suffers.
This understanding has sharpened political will to tackle the leading causes of early death. Policymakers have identified priority disease areas for intensive intervention: cancer, cardiovascular disease, neurological conditions (e.g., stroke), uro-nephrology and maternal health (i.e., 4+1: 4 major non-communicable disease areas cancer, cardiovascular, neurological, uro-nephrology + maternal health). Nationwide screening programs have been launched for cancers and heart disease to catch illnesses early. More recently, the government began offering comprehensive medical checkups to JKN members.11 The rationale is straightforward: Prevention and early treatment save lives — and money — down the line, and checkups monitoring patients control long-term healthcare costs.
2. Addressing the human resource bottleneck
To expand healthcare capacity, the government is investing directly in infrastructure and manpower. Indonesia has secured a multibillion-dollar commitment from the World Bank to fund hospital infrastructure and equipment upgrades.12 These funds are being used to procure high-cost medical equipment (e.g., imaging machines, radiotherapy units) for both new and existing hospitals.
But the government also recognizes that equipment is useless without skilled professionals. As described earlier in this piece, Indonesia has suffered from a shortage of doctors and specialists.
The Health Ministry has started sending Indonesian doctors abroad for subspecialist training, notably to China.13 These doctors are expected to return and help ease the specialist supply bottleneck. Over the next decade, this initiative should significantly expand the pool of surgeons, cardiologists, oncologists, and other specialists needed to staff new service lines in hospitals. To generate additional specialists, hospital-based specialist training has been introduced as an alternative to medical school-trained specialists. For investors, this is a critical de-risking measure: The human capital constraint is being addressed at the highest policy level.
3. Reforming the BPJS class system
Another key policy reform could significantly improve private hospital economics: the standardization of BPJS hospital bed classes. Currently, JKN offers tiered inpatient classes (Class I, II, III), each with different amenities. The government is planning to abolish these distinctions, creating a uniform standard of care for all insured patients.14
This change will essentially downgrade higher-income JKN members within the system — everyone will receive the same basic ward-level accommodation. While this may cause some dissatisfaction, it is likely to encourage those who can afford it to shift toward higher-premium private hospitals, where they can access better amenities and faster care outside the constraints of standardized JKN coverage.
For private hospital operators, this is a compelling opportunity as it may drive more affluent patients to opt for fully private care if they seek VIP-level comfort.
For hospital investors, this shift means more diagnoses and referrals that ultimately increase demand for hospital services. It creates a virtuous cycle: Early detection brings patients into the system earlier, improving outcomes and boosting volumes for providers.
Outlook: Healthy returns beyond the short term
Indonesia’s hospital sector is on the cusp of a sustained upswing, backed by fundamental demographic and epidemiological trends as well as deliberate policy support. In the near term, investors may have some concerns around BPJS reimbursement rates and operational challenges — indeed, margins on government-paid patients are tight, and private operators must adapt to a still-evolving regulatory environment. However, the long- run trajectory is clearly positive. The combination of extraordinary demand growth (from an increasingly insured population) and improving ecosystem fundamentals (more doctors, better insurance mechanisms, government funding for infrastructure) makes Indonesia a compelling healthcare investment destination. Private hospital operators who establish a strong foothold now — whether in the value-driven mass market or the higher-end specialty segment — can build scale and expertise that will be difficult to replicate later. They will also be well placed to benefit as efficiencies improve and any future adjustments in tariff or copay policy take effect. It bears noting that many private Indonesian hospitals already enjoy margins above global averages due to the supply-demand imbalance; as the system becomes more streamlined, even incremental improvements in payer mix or pricing could translate to outsized profit growth.
Investors with an eye on global trends should recognize that success in Indonesia not only yields direct returns but also positions them to export those insights to new markets on the cusp of healthcare transformation. In summary, while challenges in Indonesian healthcare remain, the direction of travel is clear and favorable. For investors willing to look past the immediate growing pains, Indonesia’s hospital sector offers a rare opportunity to do well by doing good — profiting from enabling millions of people to live healthier, longer and more productive lives. The prognosis is excellent: Indonesia’s healthcare inflection point is here, and the time to invest is now.
L.E.K. Consulting is a registered trademark of L.E.K. Consulting LLC. All other products and brands mentioned in this document are properties of their respective owners. © 2025 L.E.K. Consulting LLC
Endnotes
1WHO (2024), Executive Summary
2Asia Pacific Observatory on Health Systems and Policies (2017), p115
3GovInsider (2024)
4World Bank Group (2019), p54
5BRI Equity Research (2025), p1
6Ion Beam Applications (2020)
7Muharram et al., (2024)
8Bali International Hospital a. (2025)
9Bali International Hospital b. (2025)
10International Travel and Health Insurance Journal (2024)
11Ksatria Medical Systems (2023)
12World Bank Group (2025)
13Xinhua (2025)
14Kompas (2025)