Obesity as proof point: How GLP-1s redefined what is possible
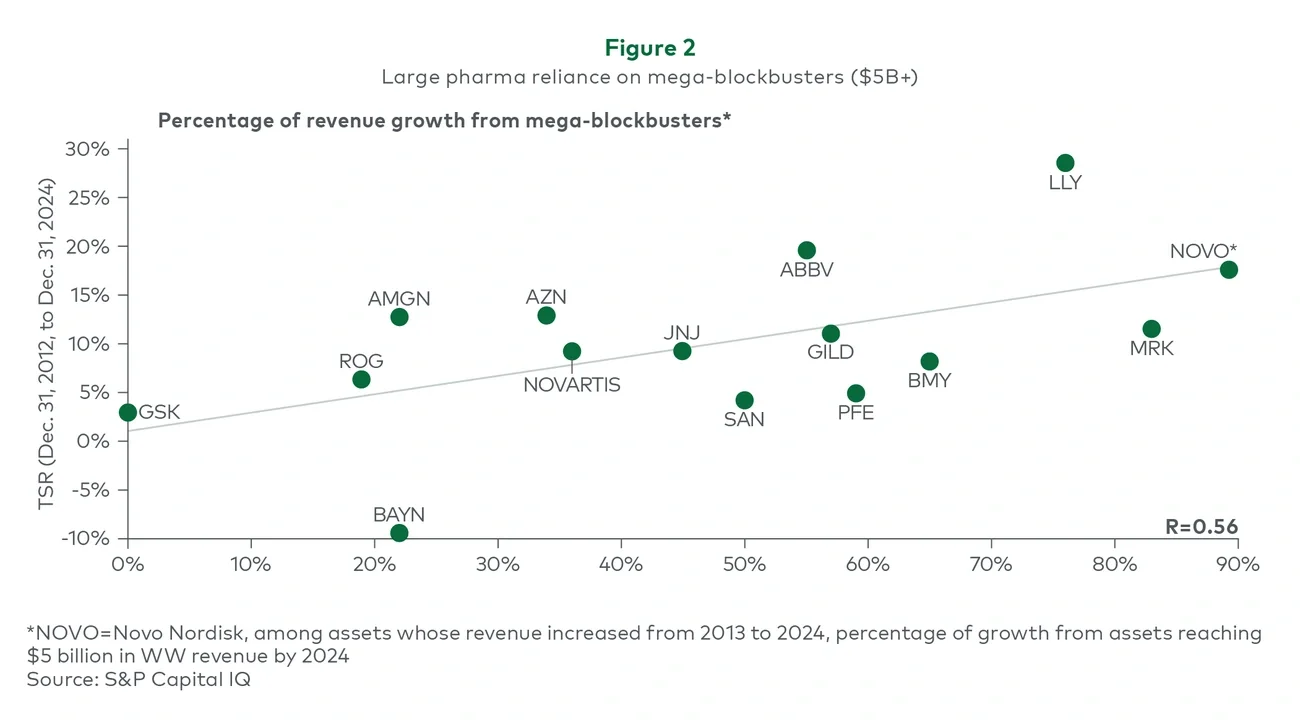
Few therapeutic areas illustrate this shift more clearly than obesity.
For decades, obesity was widely viewed as commercially unattractive: Early products suffered from safety and efficacy issues, stigma limited physician adoption and payers resisted reimbursement absent clear outcomes data. These dynamics led many companies to deprioritize the category entirely.
Yet GLP-1–based therapies fundamentally altered the equation. Step-change improvements in efficacy combined with better safety have fueled patient demand and willingness to pay for these products even in the absence of broad reimbursement. In addition, broader health outcomes data has validated hard clinical benefits beyond weight loss, which is beginning to shift the perception of obesity from a lifestyle market into a medically anchored disease, unlocking the payer coverage required for adoption at scale.
Beyond redefining obesity’s commercial potential, GLP-1s have accelerated the build-out of direct-to-patient and cash-pay infrastructure that can support opportunities across future high-prevalence disease opportunities. Telehealth initiation, digital patient acquisition and membership-based care models have streamlined an end-to-end “self-service” healthcare platform and normalized consumers paying directly for high-value therapies when coverage is limited. This end-to-end consumer-focused platform has created a commercialization backbone that future high-prevalence products can plug into rather than building it themselves.
The companies that emerged as leaders, notably Novo Nordisk and Eli Lilly, did not succeed overnight. Their advantage was built on decades of investment in incretin science, willingness to fund long and expensive outcomes trials at risk, early commitment to manufacturing scale, and the development of consumer-centric commercial models that complemented traditional physician engagement.
While there is also a fair bit of serendipity involved, both companies were committed to investing at risk once certain clinical performance thresholds were met, despite some of the remaining pricing, access and distribution challenges.
Obesity demonstrates that prevalent diseases can produce large franchises with transformative value, but only when pharma companies fundamentally reexamine their ability to enter nontraditional spaces that may not be thought of as diseases today (e.g., aging or menopause) and rethink how they discover, develop and commercialize therapies for mass markets.
Where the next mega-blockbusters may emerge
Not every prevalent disease will become the “next obesity.” However, our analysis highlights a set of therapeutic domains that share several defining characteristics: large chronic populations, meaningful residual unmet need, emerging scientific validation, growing consumer engagement and potential to reduce total cost of care.
Five domains stand out:
- Cardiometabolic disease (e.g., obesity, type 2 diabetes, MASH, hypertension) combines massive scale with increasing biological tractability and clear links to outcomes and healthcare costs.
- Neuropsychiatric conditions (e.g., depression, anxiety, substance use disorders, sleep disorders) represent enormous unmet need, with advances in neuroscience and digital tools beginning to unlock new approaches.
- Consumer-oriented health, wellness and aesthetics (e.g., hair loss, skin health, hormonal optimization) benefit from large patient populations, strong willingness to pay and digital channels, even where payer coverage is limited.
- Women’s health (e.g., menopause, PCOS, endometriosis) reflects decades of underinvestment, rising advocacy and growing employer and societal focus.
- Diseases of aging (e.g., mild cognitive impairment, sarcopenia, sensory decline) address expanding populations with high motivation for preventive and quality-of-life interventions.
Each domain presents distinct scientific, access and commercial barriers — but collectively they represent highly plausible sources of future mega-blockbusters.
What it takes to win in prevalent disease
Success in prevalent disease markets requires capabilities that differ meaningfully from those used to win in rare disease and specialty care.
From an R&D perspective, companies must be willing to invest earlier and at greater scale, often funding large long-duration trials and outcomes studies before payer pathways are fully defined. Evidence strategies must anchor value to hard clinical and economic outcomes, not just symptom improvement. Pharma companies must also be willing to consider nontraditional markets that straddle the boundaries of aesthetics, health and wellness, and medical need, but where unmet need and patient willingness to pay are high.
Commercially, mass-market diseases demand consumer-grade engagement models. Seamless end-to-end pathways that leverage new channels, digital acquisition, telehealth platforms, new payment models and simplified distribution will be needed to complement and, in some cases, precede traditional physician-led prescribing. Pricing and access strategies must be designed for sensitivity and scale, often blending reimbursed, employer-based and cash-pay pathways.
Finally, operations and supply chains must be built — from the outset — with scale in mind. In prevalent disease categories, supply constraints can rapidly become the gating factor that determines leadership.
Strategic implications for biopharma leaders
For leadership teams planning the next decade of growth, some potential implications include:
- Rebalancing portfolios toward large, chronic diseases where scientific momentum and unmet need can support multibillion-dollar franchises
- Opening the aperture for investment to include nontraditional areas (e.g., aging) where unmet need and willingness to pay is high
- Building consumer-centric commercial capabilities alongside traditional medical and sales infrastructure
- Anchoring evidence strategies to outcomes and cost of care, anticipating payer expectations early
- Preparing manufacturing and supply chains for mass adoption, not niche uptake
- Defining clear trigger points that justify disproportionate investment as scientific and commercial risk are retired
The next wave of mega-blockbusters will not emerge by accident. They will be built by organizations willing to rethink long-held assumptions about where value can be created, to balance risk-reward trade-offs and to invest accordingly.
Contact us to find out more.