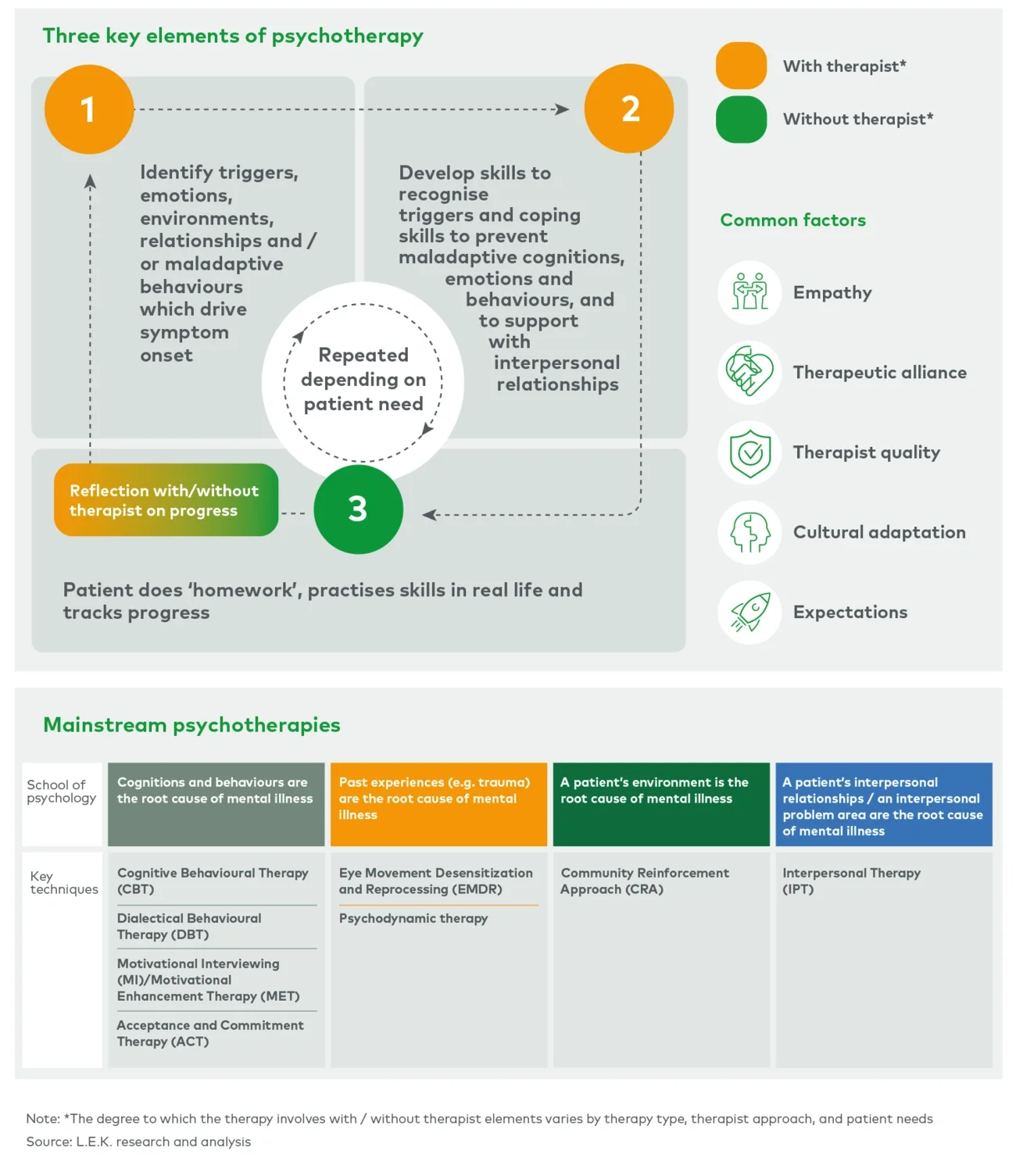
Psychedelic-assisted psychotherapy regimens sometimes use a specific therapeutic approach (such as ACT, CBT, IPT, etc.), but are typically made up of three distinct phases, and the timing and form of the psychotherapy sessions within each phase vary according to the indication and the psychedelic being used:
- Preparation phase — This can vary in total duration from approximately two to 10 hours. The objective is to set clear intentions for the treatment, introduce the psychedelic treatment model and train participants in skills that may be useful in the psychedelic experience (e.g., mindfulness, breathing exercises).
- Drug sessions — These can last between approximately 45 minutes (ketamine sessions) and eight hours (psilocybin sessions) and are usually supervised by one or two qualified healthcare professionals. Sessions may be directive, where therapists direct patients’ attention towards issues that are relevant to treatment and support them through the process (e.g., ketamine-enhanced psychotherapy for AUD or PTSD), or non-directive, where therapists only aim to keep the participants’ attention directed inwards and provide support during challenging moments (e.g., psilocybin-assisted psychotherapy for TRD, MDMA-assisted psychotherapy for PTSD).
- Integration/debriefing phase — The duration of this phase is typically two to three hours, with non-directive psychotherapy sessions occurring in the days and weeks immediately after the drug session. The objective is to process and generalise the insights gained during the psychedelic experience into the patient’s everyday life. In some treatment regimens, a greater number of directive psychotherapy sessions (e.g., CBT, motivational enhancement therapy) may occur over a period of up to six months.
Challenges of psychotherapy
A key challenge for successful commercialisation of psychedelics treatments will be to ensure that there is sufficient physical and human infrastructure to deliver the associated psychotherapy sessions. Capacity for psychotherapy is already failing to meet demand in key markets, with c.60% of therapists claiming not to have openings for new patients in the US in 2022, and growth in demand has outstripped growth of supply over recent years.
Approximately 12,000 therapists are estimated to be needed to reach peak capacity in the US for the psychedelic therapies currently in clinical development. This is expected to be feasible in the long term (c.6% of the existing c.200,000 active therapist licences), but it is likely to be challenging to meet initial levels of demand when these therapies are first launched. Therapists will require retraining to administer psychedelic-assisted therapy, which can often involve self-funding a nine-month course costing c.US$10,000 for novice therapists, or a shorter (a few days long) and lower-cost training for more experienced therapists. Furthermore, specialised clinics may need to be established to administer drug sessions as Risk Evaluation and Mitigation Strategy programmes limiting psychedelic use to certain centres may be imposed to alleviate safety concerns and improve regulator trust.
The high variability and complexity of patients, their circumstances and psychotherapy settings (i.e., the type and timing of psychotherapy sessions, quality of the therapist, etc.) in psychedelic clinical trials have created challenges for replicability and generalisability of results. This has contributed to continuing uncertainty about how psychedelic-assisted psychotherapy will be managed by insurers, medical systems and regulatory bodies.
Proposed psychedelic therapy treatment models are also time and resource intensive and therefore expected to have relatively high cost compared with current standard of care (e.g., US$11,500 for one Lykos PTSD treatment regimen versus the much lower cost of standard of care therapy such as selective serotonin reuptake inhibitors). Historically, access to psychedelics therapy has relied on a combination of patient out-of-pocket funding and via manufacturer-sponsored clinical trials. This is starting to change since the American Medical Association issued first Current Procedural Terminology (CPT) III code for psychedelic therapies, thus providing healthcare professionals some means to seek reimbursement. However, given the uncertainty about the number of treatment sessions required per patient, this relatively high cost of treatment still has the potential to create market access issues that will also need to be resolved.
Potential solutions
Successful commercialisation of psychedelics and their integration into psychiatric standard of care will require input from a wide range of stakeholders to build the market. Initiatives to address the key challenges for commercialisation could include:
- Investment in therapist quality beyond just qualifications or experience to ensure that psychedelics are appropriately administered by high quality therapists. This would help standardise the role of psychotherapy approaches, such as CBT, in psychedelic treatment regimens, and help ease the confidence of regulators / insurers in this therapeutic approach - both of which are important for commercialisation. Once therapist quality is established and the role of psychotherapy in psychedelic-assisted psychotherapy standardised, development of clear guidelines and incentives for psychotherapists to follow best practices, and implementation of training programmes based on these standardised guidelines, would also be necessary.
- Adopting digital approaches to increase capacity in the market, reduce the cost of treatment and increase standardisation of the psychotherapy element of the treatment regimen. Digital psychotherapy could be offered as an adjunct to in-person therapy, such as through a companion digital tool or additional digital psychotherapy sessions, or as a standalone, comprehensive digital patient engagement solution. Prescription digital therapeutics are already being used to deliver standardised versions of traditional behavioural therapies (e.g., Somryst CBT treatment for insomnia) and can be enhanced with artificial intelligence to deliver more personalised treatments. A number of psychedelics players, including Compass, atai and MindMed, are currently exploring a range of digital offerings.
- Using group therapy and task shifting to reduce the total number of therapists required and increase capacity in the market. Whilst this may not be appropriate for dosing sessions, group therapy sessions in the preparation and debriefing/integration phases of treatment could reduce the total number of therapists required to commercialise psychedelic therapies. Moreover, task shifting in the form of using less qualified but carefully selected staff (e.g., community health workers) to deliver psychotherapies could be used to address the shortage of professional therapists, especially in the low- and middle-income countries, where there is a limited number of specialists that need to be freed up for dealing with more complex cases.
- Personalising the number of psychotherapy sessions offered as part of the psychedelic treatment regimen. There is significant variation in the number and duration of the sessions required for each psychedelic therapy, however they are usually offered as a standardised package, which includes a fixed number of sessions. Personalised treatment regimens with varying number / duration of sessions on a case-by-case basis depending on patient needs could reduce the therapy infrastructure required to commercialise these regimens.
- Finding further evidence to determine whether psychedelics are effective treatments by themselves or whether they act as catalysts for the treatment provided by psychotherapy. Data from Compass Pathways’ phase 2 trial shows patients have a dose-dependent response to psilocybin, which indicates that psilocybin has a pharmacological effect, a finding that is critical for it to be recognised as a new treatment option in the future. If further evidence could be generated to elucidate the treatment mechanism and understand whether psilocybin is efficacious by itself as a treatment for TRD, it would potentially enable psilocybin to be administered under the supervision of a person who is not a licensed psychotherapist, solving the potential capacity challenge. Furthermore, under existing regulatory models, regulatory bodies such as the FDA review the efficacy and safety of drugs, not psychotherapies; evidence to illustrate the mechanism of action of psychedelics would therefore most likely facilitate the regulatory approval process.
Conclusion
How L.E.K. Consulting can help
As mental health assumes an increasingly prominent role in the healthcare system, we help organisations address a range of key issues, creating value for our provider clients and across the investment landscape. We assist clients with their commercial and growth strategy, supporting them in growing sectors such as psychedelic drugs. Our approach helps organisations consistently make better decisions, deliver improved business performance and create greater shareholder returns.
To find out more and for a further discussion, please contact Adrienne Rivlin, Partner.
L.E.K. Consulting is a registered trademark of L.E.K. Consulting. All other products and brands mentioned in this document are properties of their respective owners. © 2024 L.E.K. Consulting
Endnotes
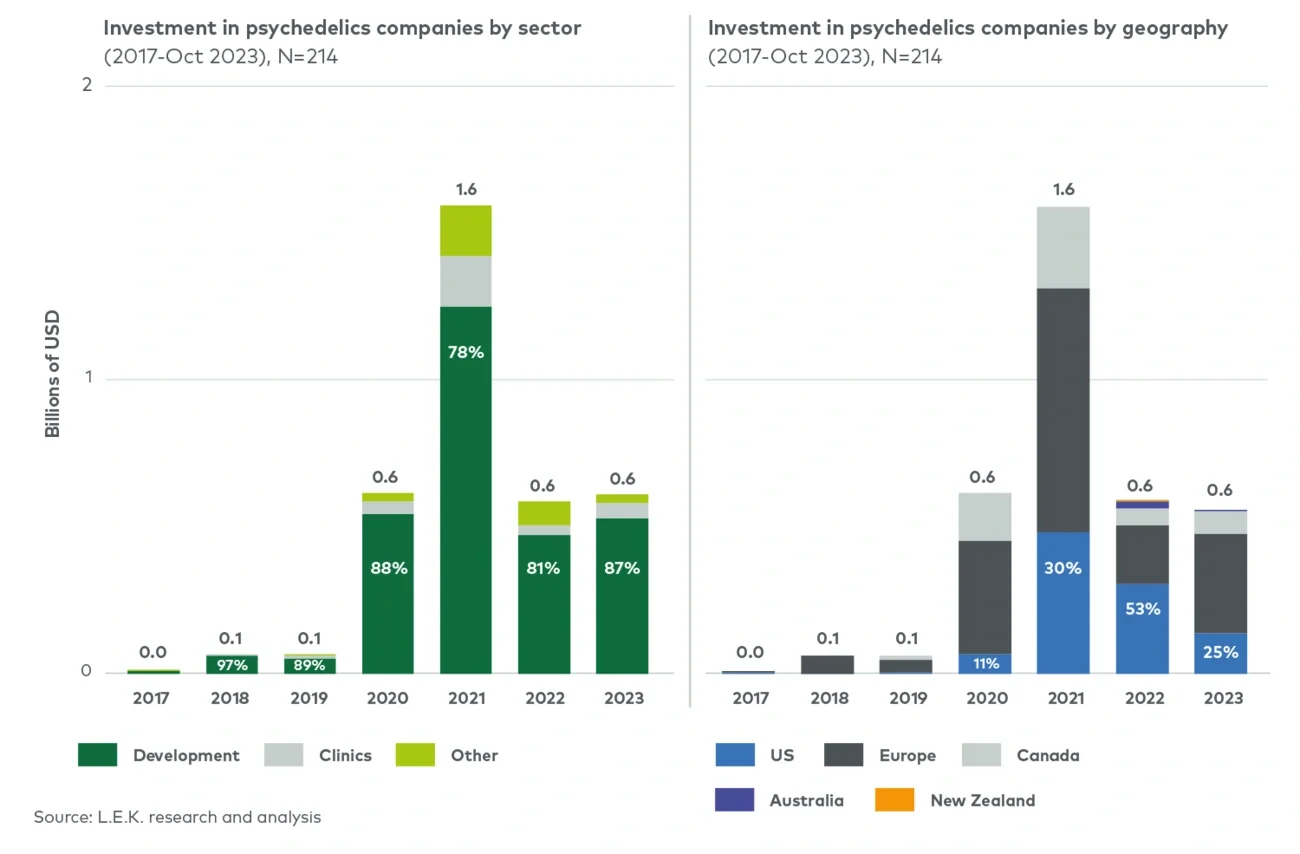
1L.E.K. Consulting Executive Insights, Exploring the Psychedelics Landscape: Looking Ahead to Funding in 2024 ...
2MarketWatch; Data Bridge Market Research; Market Industry Reports; Research and Markets
3NIDA; Journal of addiction medicine
4Wampold, 2015
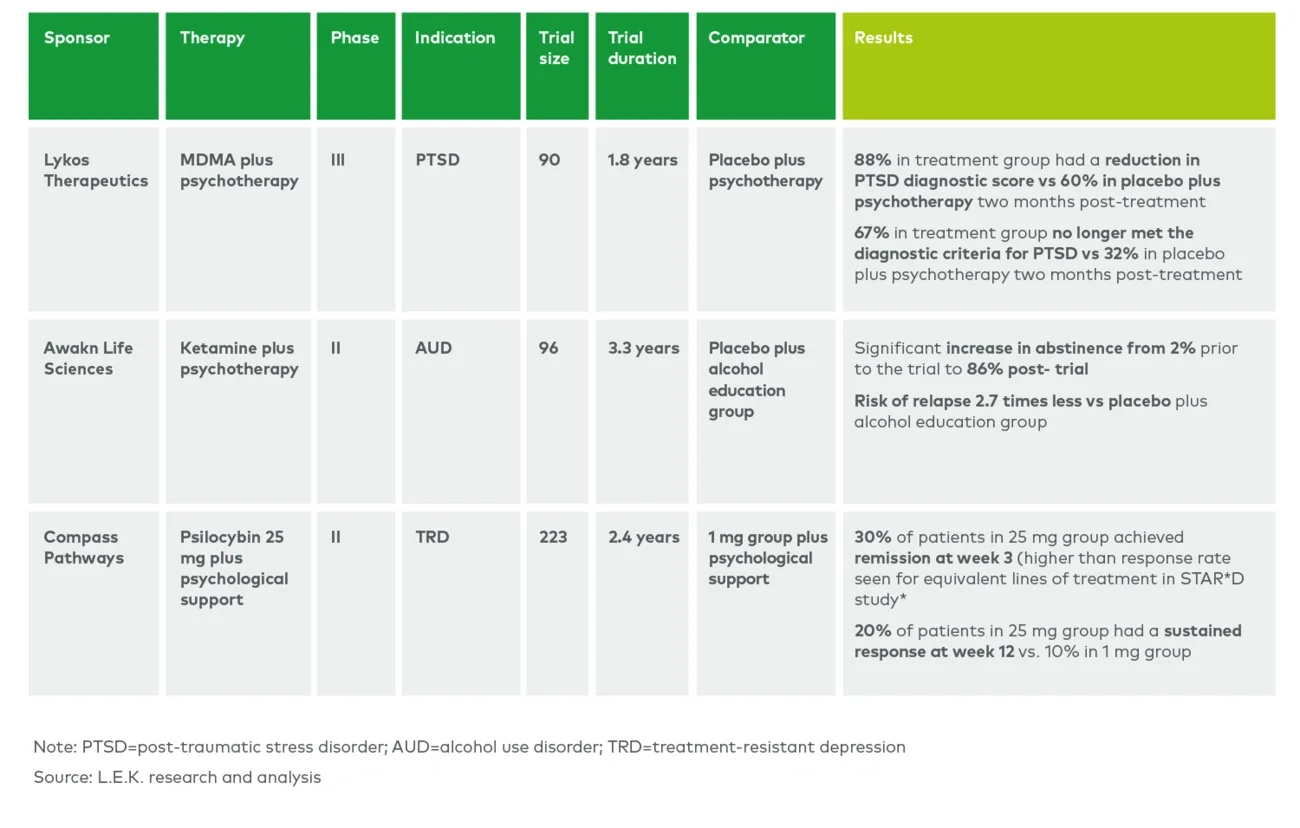
5Clinicaltrial.gov; L.E.K. research and analysis
*Clerkenwell health are a contract research and psychedelic-assisted therapist training organisation