The COVID-19 pandemic (2020-22): The changing nature of demand
COVID-19 further stressed a system already facing a nurse shortage.
-
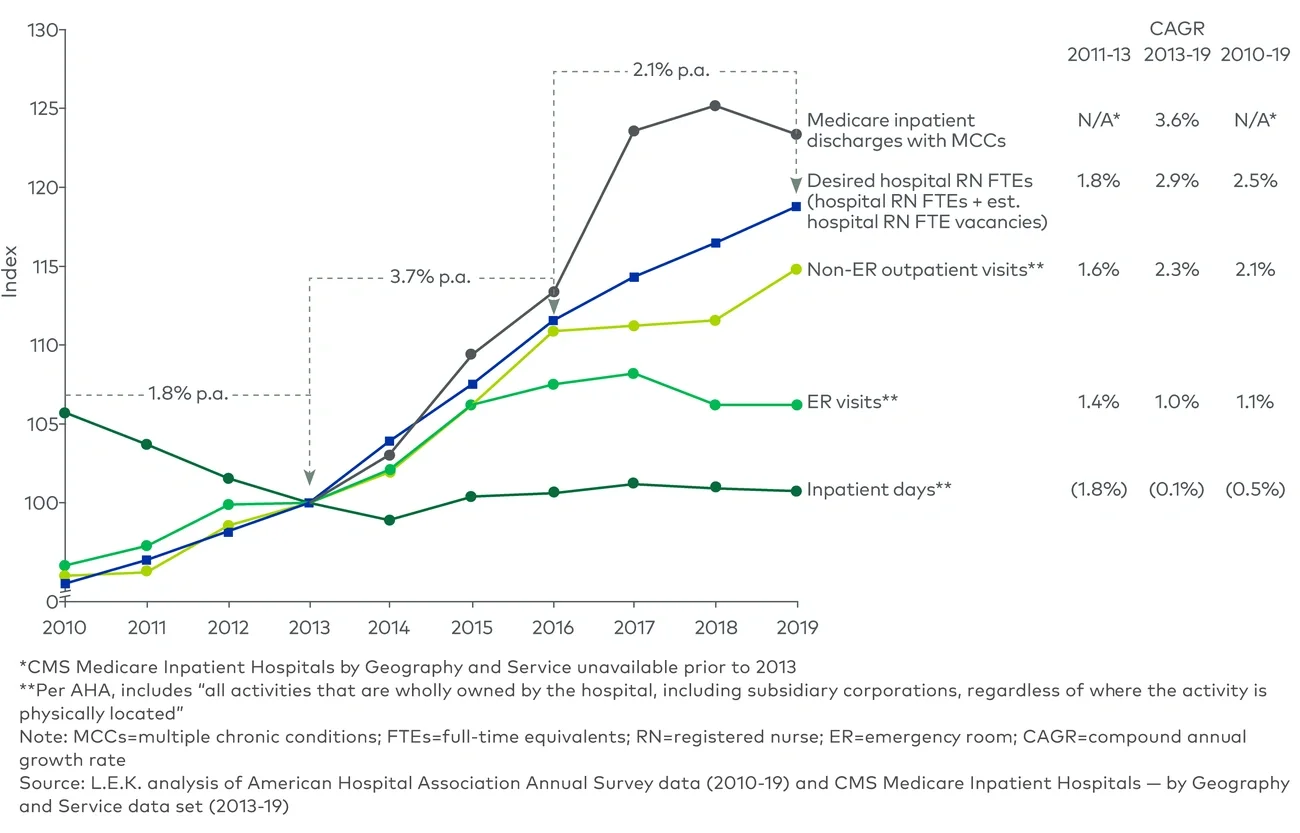
In 2020, hospital utilization declined across ER visits, non-ER outpatient visits and inpatient days as non-COVID-19 patients avoided seeking care and hospitals canceled or reduced elective procedures15
-
The crisis level of demand for COVID-19 care led hospitals to redeploy some of their workforce from their current departments to intensive care/COVID-19 units16
-
In 2021, ER visits remained more than 10% lower than 2019 levels, inpatient days rebounded to 2019 levels and non-ER outpatient visits rose to 2.7% higher than 2019 levels, indicating that volume had largely returned to pre-pandemic norms17
Historical context: The nurse population, or ‘supply’ (2010-2022)
Prior to COVID-19 (2010-19): Growth despite constrained nurse education capacity
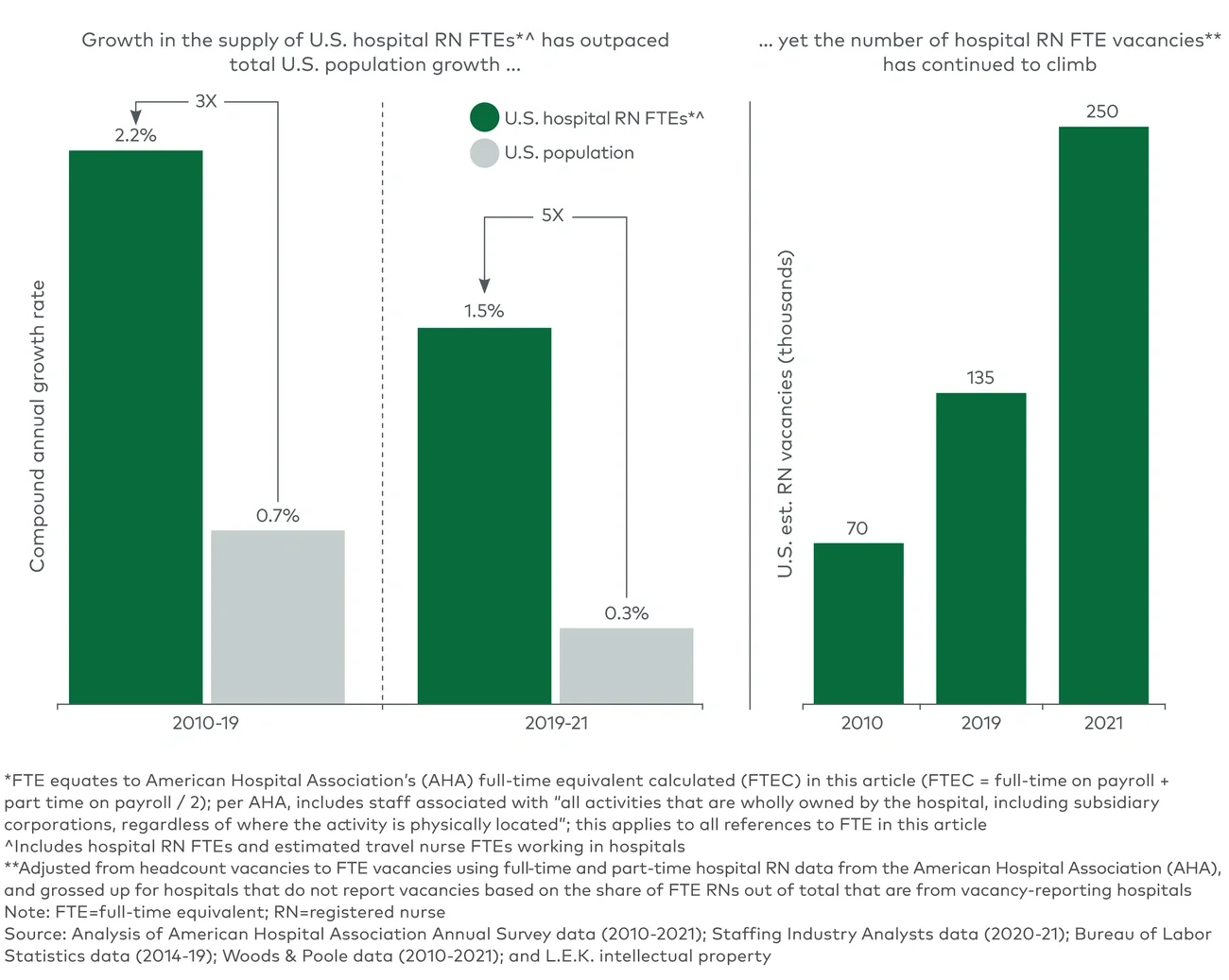
Unlike what a casual observer might expect, the size of the U.S. RN workforce in fact increased every year since at least 2008, growing from approximately 2.7 million in 2010 to approximately 3.2 million in 2019 (2.2% CAGR).18 Similarly, the number of RN FTEs working at hospitals increased from about 1.5 million in 2010 to about 1.8 million in 2019 at a 2.2% CAGR.19
Nurse population growth is a function of two factors: new entrants into and exits from the profession. While the number of entrants into the workforce (those who passed the National Council Licensure Examination for RNs (NCLEX-RNs)) grew 2.3% annually from 2010 to 2019 — up to about 170,000 by 201920 — a lack of training capacity, largely driven by faculty shortages,21 constrained growth. In 2019, for example, approximately 68,000 qualified applications (not applicants) were rejected from entry-level baccalaureate nursing programs for that reason.22
Given the constraints on training, exits23 from the profession are the primary driver of total nursing capacity. From 2010 to 2019, 2.5% of RNs left the profession each year on average.
The COVID-19 pandemic (2020-22): Spike in exits exacerbates shortage
U.S. RNs were on the front lines of the COVID-19 pandemic and faced severe, countless challenges. A 2021 survey found that approximately 75% of surveyed nurses across care settings felt stressed and about 62% felt overwhelmed.24 The survey also indicated that approximately 50% of nurses stated they intended to (21%) or might (29%) leave their position in the next six months. A reason cited by nearly half of those intending to leave was the negative effect of work on their health and well-being.
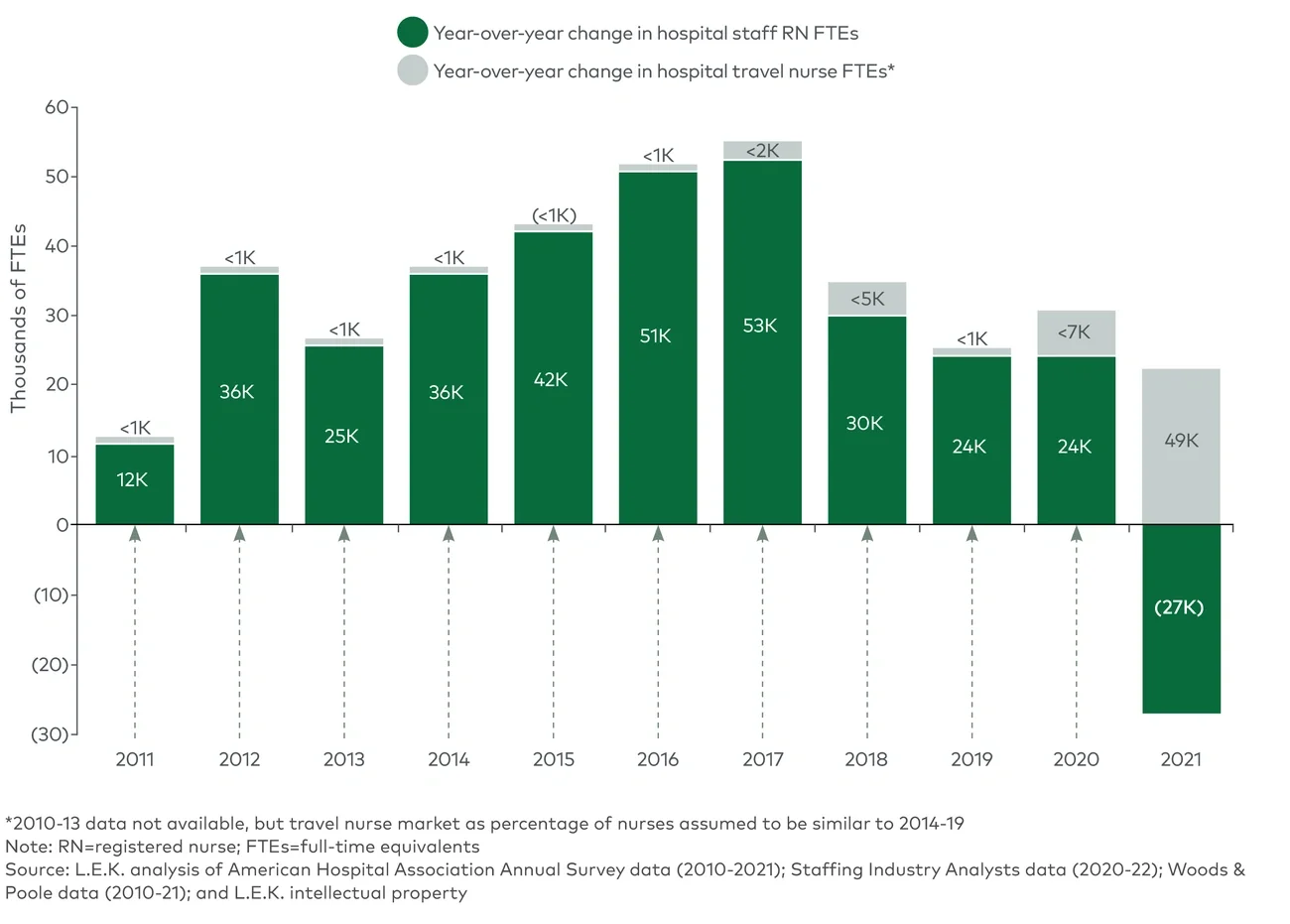
Many did leave, and exits from the profession spiked relative to historical norms. According to American Hospital Association (AHA) data, hospital staff RN FTEs declined by 1.5% in 2021,25 the only decline in the 2010-2021 period (see Figure 3). That same year, estimated hospital RN FTE vacancies increased by nearly 70%, reaching about 250,000.26 And from 2021 to 2022, enrollment in bachelor of science in nursing (BSN) programs declined by 1.4%, the first year of decline since 2000.27
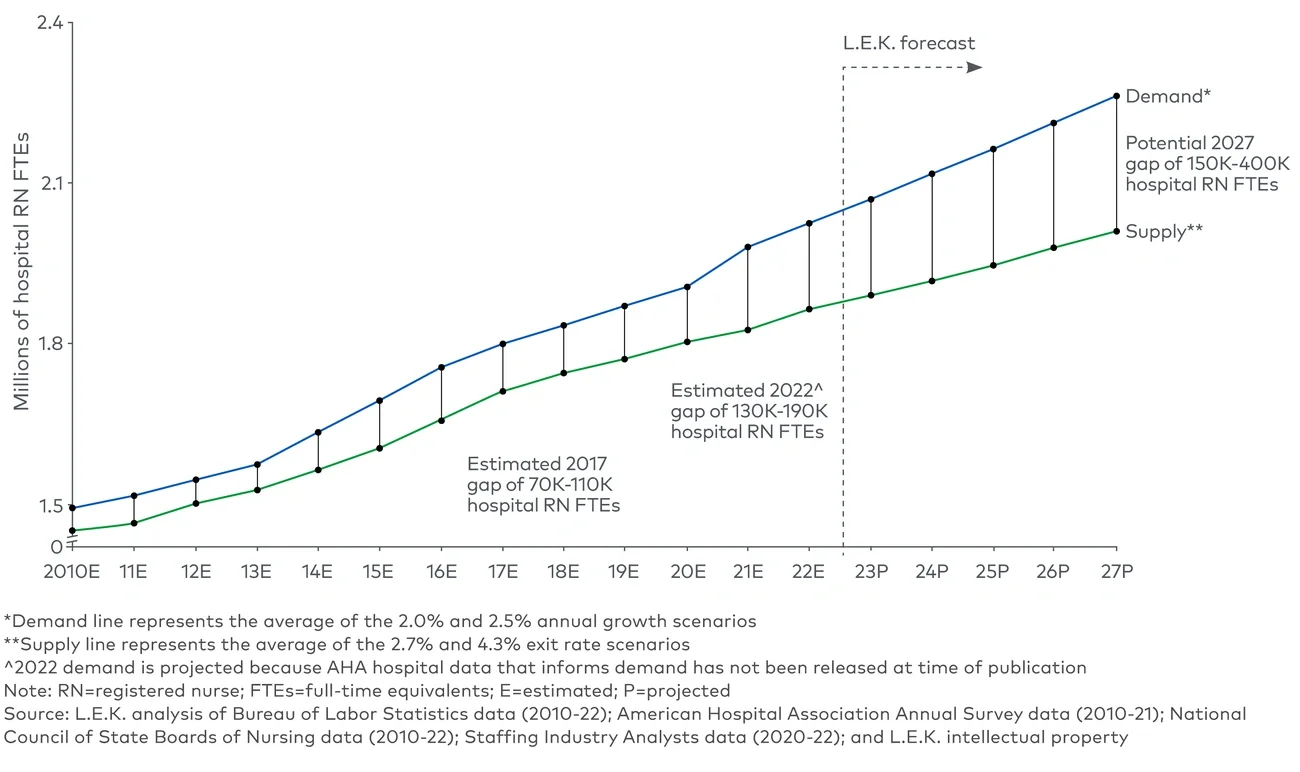
During this time, hospitals sought out travel nurses to supplement their supply of nurse staff. The travel nurse market28 grew to $27.6 billion in 2021, nearly tripling from the prior year.29 There were 30,000 to 40,000 hospital travel nurse FTEs in 2019, compared with 90,000 to 100,000 in 2021 and 120,000 to 140,000 in 2022.30 L.E.K. Consulting’s analysis of historical supply and demand data suggests that even after adding travel nurses to the hospital RN supply, the U.S. hospital RN shortage reached approximately 150,000 FTEs in 2021, up from 80,000 to 120,000 in 2019.
Data from staffing company Vivian Health suggests that as of late 2022, average U.S. travel nurse pay had fallen from its early 2022 peak as some of the most acute COVID-19-related drivers subsided, but the amount is still significantly elevated relative to pre-pandemic levels.31