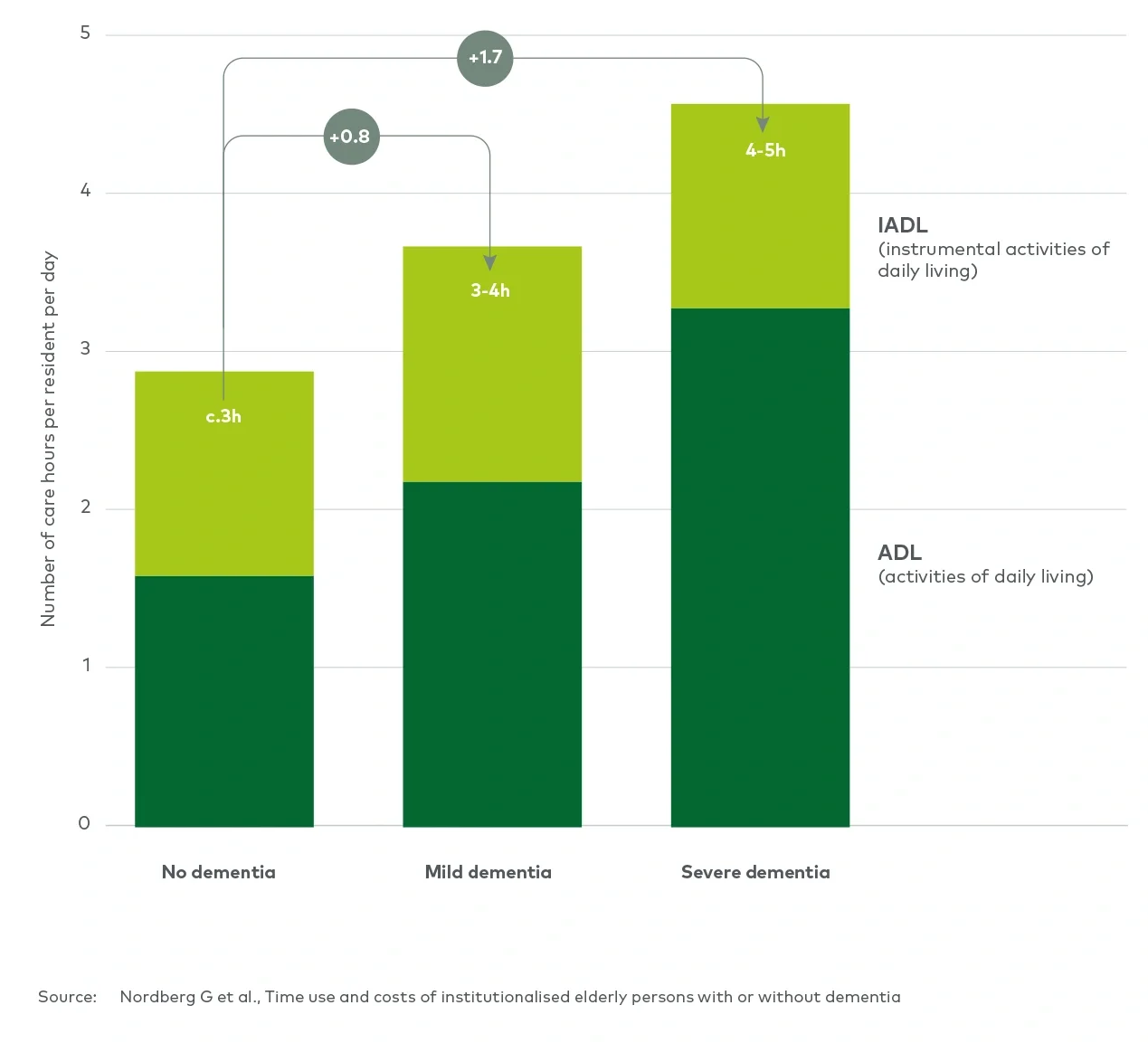
Concerned about the higher care requirements and worried about inability to recoup sufficient fees, many providers make the natural but unfortunate response to prioritise segments of the market which are more economically viable (e.g. self-funders and public- funders with mild dementia) and increasingly turn away referrals for individuals with more advanced dementia.
Conclusion: concerted efforts are needed to address the dementia challenge
Dementia is a global health challenge that requires concerted efforts from individuals, governments, and health and social care providers. The care home industry plays a crucial role in the dementia care pathway, catering to those who have more advanced cognitive impairments and/or behavioural and psychological symptoms.
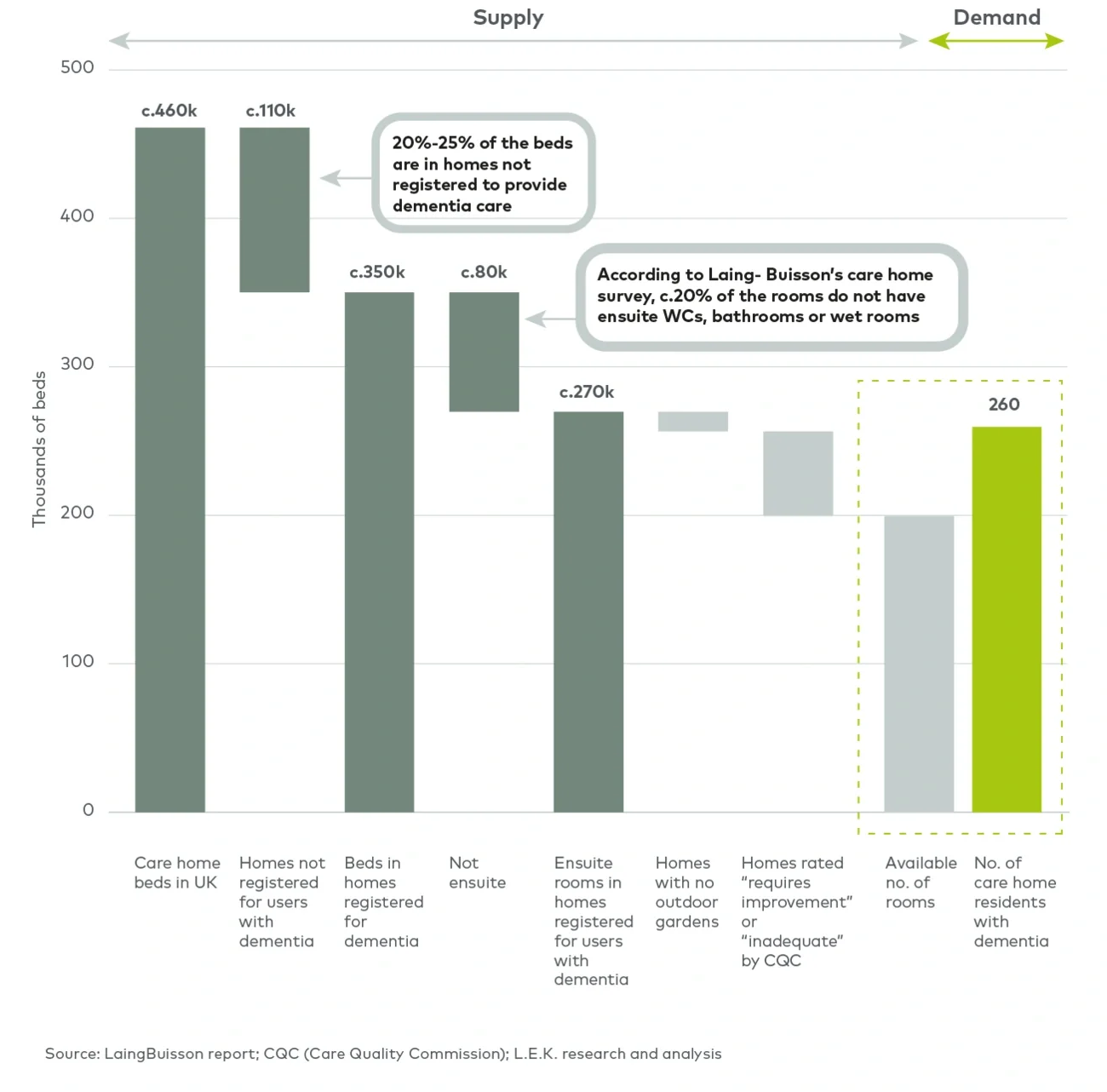
However, our analysis reveals a concerning gap between the supply of fit-for-purpose care home places and the increasing number of people with dementia requiring residential stay. This supply shortage is in part the consequence of prolonged public funding shortages and inability of councils to fund dementia care adequately. Providers naturally choose to focus on customer segments with lower needs and better economics, steering away from individuals with more profound behavioural and cognitive symptoms of dementia. Regrettably, those individuals who are turned away most often happen to be those with the fewest options — their behavioural symptoms make it impossible for family and carers to safely look after them at home, yet the conditions are not severe enough to warrant stays in mental health facilities or hospitals.
In light of these challenges, it is evident that a coordinated national strategy is needed to address the rising demand for dementia care. However, as the political parties gear up towards the general election, the topic of dementia seems to have taken a backseat. Nevertheless, efforts by individual care home providers can still make meaningful impacts in responding to the needs of residents with dementia and shaping the sector. As a minimum, providers need to scrutinise their own network and customer base to record, track and analyse care requirements and the changes over time in a bid to demonstrate outcome and value for money for cash-strapped local authorities. Care home providers, large and small, need to develop their own dementia strategy. There is no one-size-fits-all solution, and providers must consider their unique circumstances and ambitions.
How L.E.K. can help
To support providers as they navigate the challenges of dementia care, we can offer tailored advice backed by rigorous analysis and deep understanding of international best practices. For example, we performed a comprehensive catchment analysis for a specialised dementia care provider to quantify the addressable and serviceable market within its network. The client gained a better understanding of the quality of their portfolio and attractiveness of catchment areas to tailor future growth strategy. To discuss your needs, contact us.
L.E.K. Consulting is a registered trademark of L.E.K. Consulting LLC. All other products and brands mentioned in this document are properties of their respective owners. © 2024 L.E.K. Consulting LLC
Endnotes
1 Yang HD, Kim DH, Lee SB, Young LD. History of Alzheimer’s Disease. Dement Neurocogn Disord. 2016 Dec;15(4):115-121. doi: 10.12779/ dnd.2016.15.4.115. Epub 2016 Dec 31. PMID: 30906352; PMCID: PMC6428020.
2 Raphael W, Bo H, Luis BA, Amritpal R. Projections of older people with dementia and costs of dementia care in the United Kingdom, 2019- 2040. Care Policy and Evaluation Centre, London School of Economics and Political Science.
3 Afram B, Stephan A, Verbeek H, Bleijlevens MH, Suhonen R, Sutcliffe C, Raamat K, Cabrera E, Soto ME, Hallberg IR, Meyer G, Hamers JP; RightTimePlaceCare Consortium. Reasons for institutionalization of people with dementia: informal caregiver reports from 8 European countries. J Am Med Dir Assoc. 2014 Feb;15(2):108-16. doi: 10.1016/j.jamda.2013.09.012. Epub 2013 Nov 12. PMID: 24238605.
4 William L. Care homes for older people. 33rd edition.
5 Knight Frank. UK Care Homes Trading Performance Review 2023.
6 Care England. Sector Pulse Check 2023. January 2024.
7 William L. Care homes for older people. 33rd edition.
8 Nordberg G, Wimo A, Jönsson L, Kåreholt I, Sjölund BM, Lagergren M, von Strauss E. Time use and costs of institutionalised elderly persons with or without dementia: results from the Nordanstig cohort in the Kungsholmen Project: a population based study in Sweden. Int J Geriatr Psychiatry. 2007 Jul;22(7):639-48. doi: 10.1002/gps.1724. PMID: 17225239.