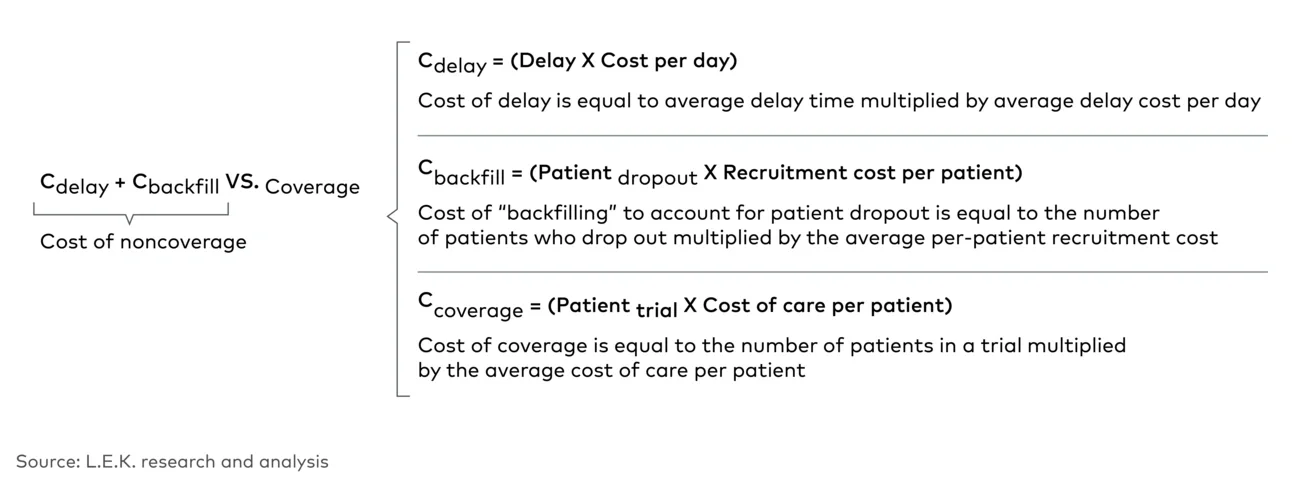
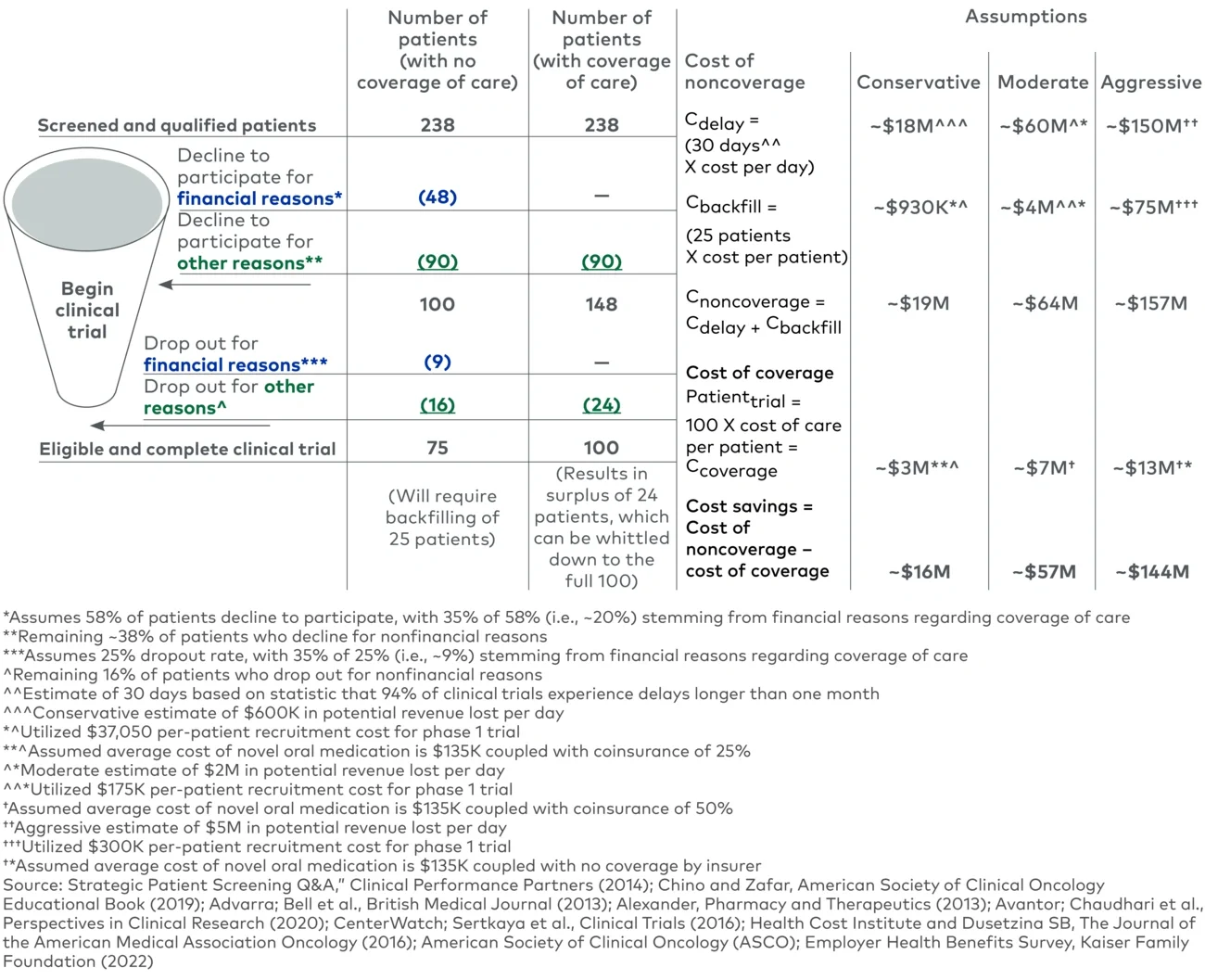
In the moderate example scenario where a sponsor does not provide coverage of baseline therapy, we can see that to begin a clinical trial with 100 patients, the sponsor must start with a much larger pool of screened and qualified patients, to account for patients who decline to participate. After the trial begins, around 9% of participants will drop out for financial reasons, with additional dropout for nonfinancial reasons. Ultimately, the trial will have 75 patients who are eligible and complete the trial, but it will require backfilling of 25 patients. Considering the cost of backfilling and the delays associated with this, the total cost to the sponsor of noncoverage is about $64 million.
If the sponsor were to provide coverage of baseline therapy, it would reduce the number of patients declining to participate for financial reasons to zero, expanding the number of patients who begin the clinical trial to 148. Additionally, over the course of the trial, no patients would drop out for financial reasons, resulting in 124 patients who would be eligible and could complete the trial. This could allow the sponsor to further screen those patients and ensure that 100 patients complete the trial. However, we must account for the per-patient cost of baseline therapy for the clinical trial; assuming that all patients receive baseline therapy and only require coverage of out-of-pocket expenses, the cost would be approximately $7 million.
If we compare the cost of coverage versus noncoverage, the apparent cost savings is roughly $57 million. The bulk of these savings stems from eliminating the delays that a clinical trial would experience, ultimately affecting the sponsor’s time to launch. Using more conservative or aggressive assumptions, adjusting the amount of out-of-pocket cost a patient may face, and using the logic laid out previously, the sponsor may be able to drive cost savings ranging from about $16 million to about $144 million.
It is important to note that this is an illustrative example that makes various assumptions regarding size of trial, delays in timeline, lost revenue and cost of baseline therapy. There is a point at which a trial size may become too large, the cost of coverage of baseline therapy may be too prohibitive or the projected revenue of the therapy in development is not as large. However, there are cases in which sponsor coverage of baseline therapy will be worthwhile due to projected savings. At the outset of any trial planning processes, sponsors should assess the overall cost/benefit analysis and explore all potential options available to drive better outcomes.
A case for coverage
As shown, for an early-stage oncology trial, there is clear potential for cost savings for sponsors that elect to cover the cost of care for trial participants. In addition to the financial benefits, there are other benefits such as improving trial participation and reducing dropout (e.g., only 90 patients declining to participate versus 138).
Recruiting for clinical trials may also improve as screened and qualified patients who previously may have dropped out for financial concerns or access barriers related to baseline or standard of care therapy would be more likely to be retained as their care would be covered fully with no significant out-of-pocket expenses or surprise costs. As financial barriers are removed and the pool of patients increases, sponsors may be able to reduce the number of trial sites, further increasing cost savings (site costs, excluding personnel, have been estimated to range from about $400,000 to roughly $3 million). Furthermore, there are “soft” or intangible benefits of covering cost of care, including improvement of sponsor perception as a “sponsor of choice”; supporting access to care among a broader, more diverse group of patients; enabling patients to help move therapy innovation forward for those to come; and improving timelines for therapy development.
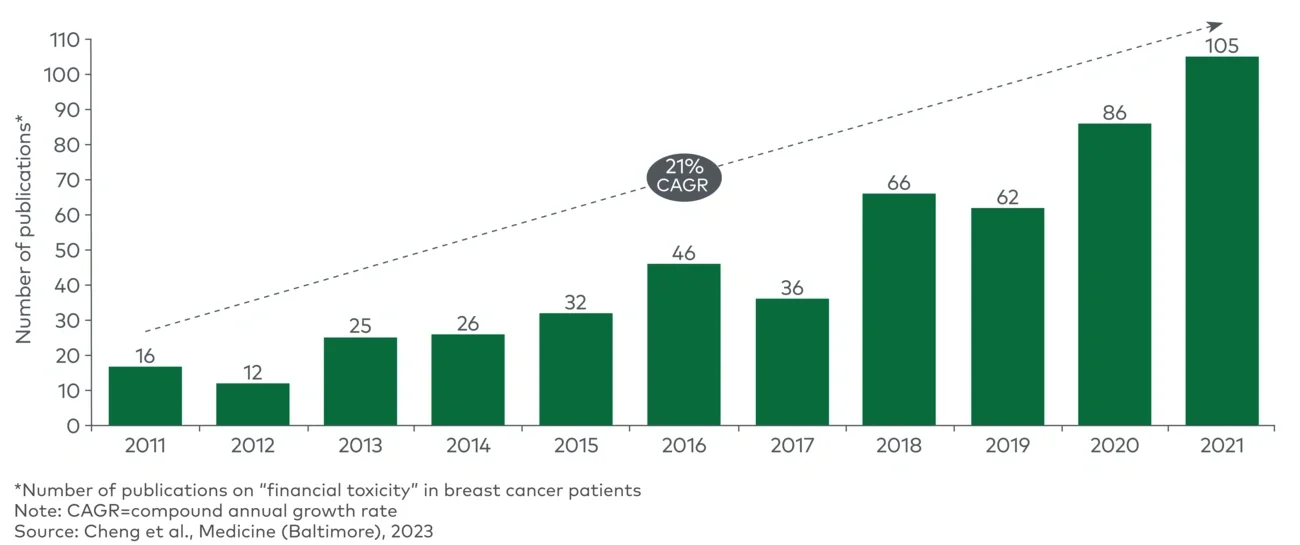
Overall, participation in clinical trials remains limited. While several solutions are being explored (e.g., improving access/education, alleviating indirect expenses), one area that is gaining additional attention is the financial strain that participation in trials may place on patients. Patients are concerned about lack of or lapses in insurance coverage. By opting to cover baseline therapy for trial participants, sponsors may be able to drive approximately $16 million to $144 million in cost savings per 100 patients through mitigation of trial delays and eliminating the need for backfilling while also improving their reputation as a sponsor of choice. Beyond benefits to sponsors, there are a host of benefits to patients who can stay in trials without fear of financial burden and help drive medicine forward for those who come after them.
For more information, please contact lifescience@lekinsights.com.
L.E.K. Consulting is a registered trademark of L.E.K. Consulting LLC. All other products and brands mentioned in this document are properties of their respective owners. © 2024 L.E.K. Consulting LLC