The value proposition
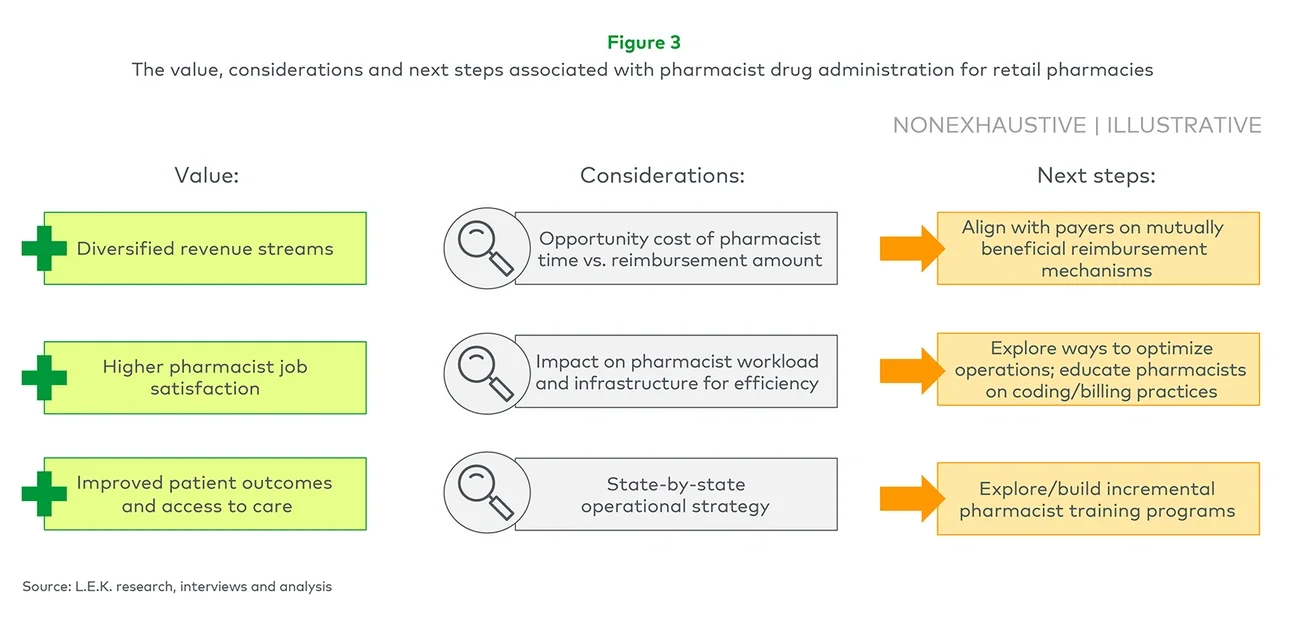
Pharmacist drug administration can bring value to retail pharmacies in multiple ways:
-
Additional revenue and margin — Diversifying services beyond script fills enables pharmacies to capture new revenue streams and potentially offset declining margins.
-
Higher pharmacist job satisfaction — Greater time spent on clinical activities has a direct correlation to higher pharmacist job satisfaction. Some pharmacists have said they regarded vaccine administration during COVID-19 as one of the most rewarding experiences of their lives.
-
Better patient outcomes — Pharmacist-led community interventions can improve patient adherence to medications and contribute to better management of health complications. For example, states that allowed greater pharmacist oversight of PrEP saw a 110% usage increase in the two years following the policy changes as compared to the year the policies were implemented.
-
Improved access to care — In the U.S., 90% of people live within 5 miles of a retail pharmacy, and in a 2022 survey, 53% of respondents said they would go to a pharmacy for healthcare services.
Key considerations
Before enabling pharmacists to administer drugs, retail pharmacies need to take a host of factors into consideration prior to execution:
-
Time vs. money — Pharmacies should analyze the potential opportunity costs of redirecting pharmacists’ time from so-called normal workflow activities to administering injectables, which currently have an undetermined reimbursement amount and structure.
-
Pharmacist workload and support — Given the shortage of pharmacists and other workforce strains, pharmacies may need to invest in more advanced technology and efficient infrastructure (e.g., IT automation solutions, additional support staff, remote pharmacist supervision where legal) to lighten the administrative workload of existing pharmacists prior to introducing drug administration to their routine workflow.
-
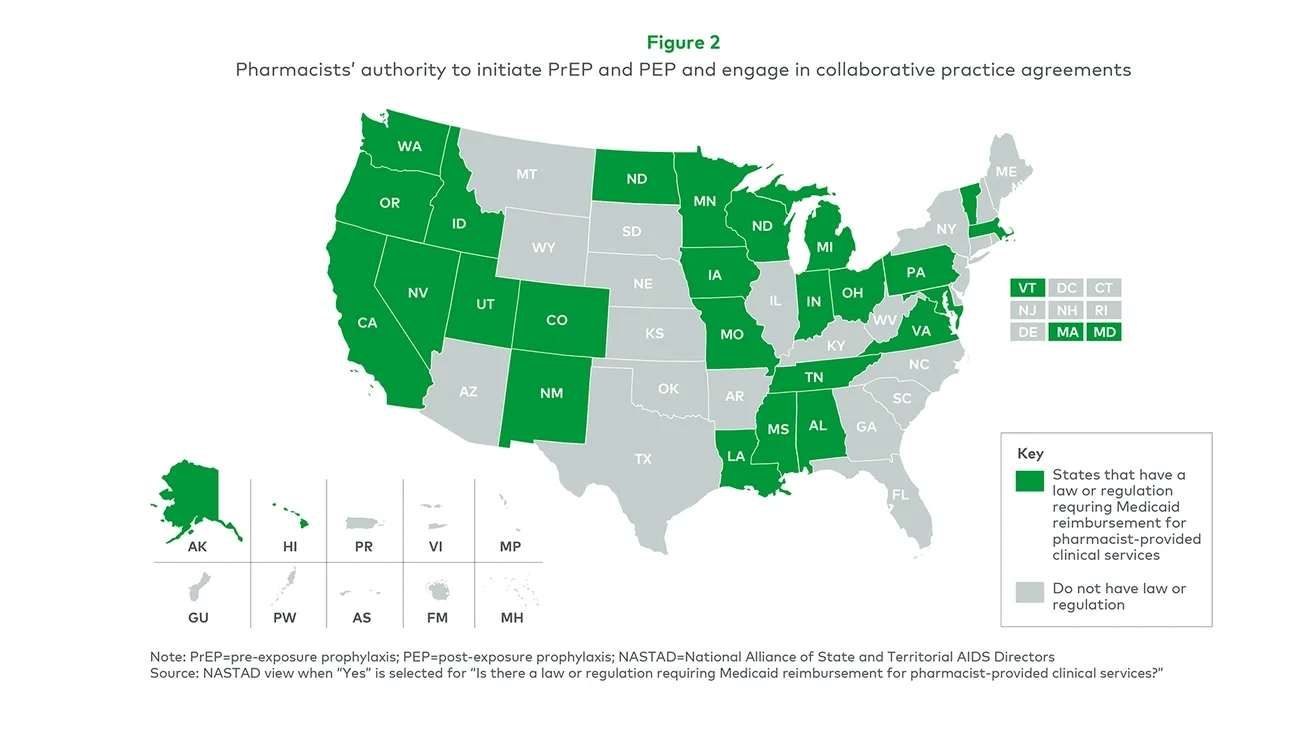
State-level operational strategy — National retail pharmacies likely need a state-by-state strategy, as state policies regarding pharmacists’ scope of practice and reimbursement requirements vary.
Next steps to take
Once the potential value of pharmacist drug administration is clear, and the related key considerations are acknowledged and addressed as needed, retail pharmacies need to take some crucial next steps:
-
Payer alignment — Most commercial payers have yet to develop reimbursement processes for pharmacist drug administration, and with no benchmark from an entity to set rates the way, for example, the Centers for Medicare & Medicaid Services establishes a physician fee schedule, establishing standards is challenging. Aligning with payers on mutually beneficial reimbursement mechanisms is key.
-
Optimization of operations plus education — With inconsistent billing practices for drug administration, pharmacists may lack familiarity with or may be uncertain about how to bill for services such as drug administration outside of their traditional scope. Optimizing operations will reduce pharmacist time spent on administrative tasks, as will educating pharmacists on coding and billing practices.
-
Additional pharmacist training — States such as Illinois and California have rolled out training requirements, and some pharmacy schools have begun offering drug administration in their curricula, but it is not yet widespread. Incremental training programs will help pharmacists get up to speed.
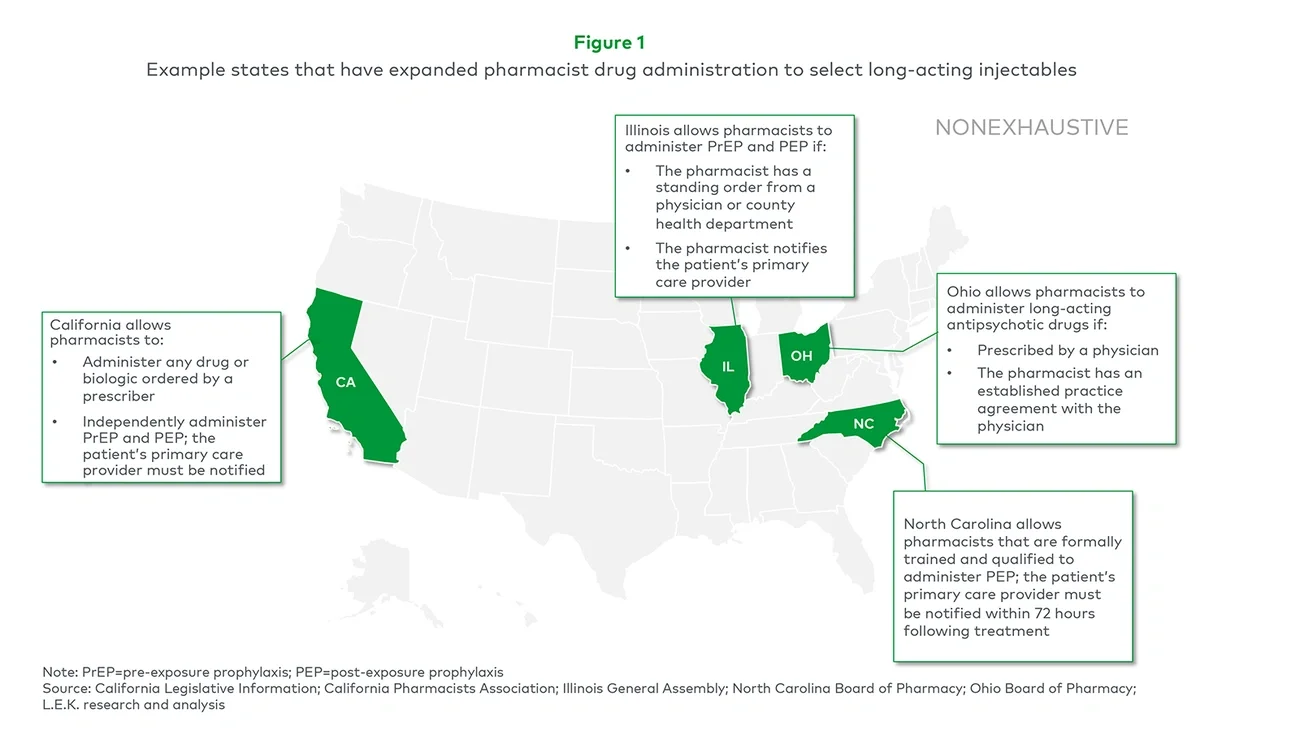
State of the industry
While retail pharmacies have yet to widely incorporate drug administration into their routine services, some have begun to take advantage of policy changes to begin implementing it.
For example, in 2022, Albertsons formed a collaborative practice agreement with Montana-based telepsychiatry practice Frontier Psychiatry, by which Albertsons’ pharmacists can administer LAIs for mental health conditions and substance abuse disorders. Hayat Pharmacy, a local retail pharmacy chain in Wisconsin, formed a similar partnership program with a psychiatric clinic. Within the first year, Hayat pharmacists administered an average of 24 LAIs per month in addition to traditional script fills and secured per-LAI gross margins ranging from $30 to $125.
Looking ahead, as pharmacist drug administration becomes more prevalent, retail pharmacies will need to evaluate the following factors:
-
Potential contract negotiation levers — The ability to negotiate favorable contracts and rates with payers will depend on pharmacies being able to demonstrate a significant volume of patients.
-
Reimbursement mechanisms — As more state legislation is passed requiring payers to reimburse for the service, monitoring developments in reimbursement mechanisms and strategizing based on how fee structures and benchmark rates materialize will be key.
-
State-by-state prioritization — Every state regulates the practice differently, so pharmacies will need to use a go-to-market roadmap to prioritize where to first roll out the service while ensuring all of its rollout locations are tailored to support it.
-
Potential synergies with existing services — As some states only allow pharmacist drug administration under physician supervision, retail pharmacies will need to assess their existing infrastructure (e.g., CVS and Walgreens already employ physicians to support retail clinics) and evaluate potential provider partnerships to address any gaps.
L.E.K. Consulting’s Healthcare Services practice continues to perform work across this space to help clients navigate uncertainties and growth opportunities. With our knowledge and expertise, we can help develop strategic solutions that not only fit your needs for commercial excellence but also for growth in the years ahead.
For more information, please contact healthcare@lekinsights.com.
L.E.K. Consulting is a registered trademark of L.E.K. Consulting LLC. All other products and brands mentioned in this document are properties of their respective owners. © 2023 L.E.K. Consulting LLC