

India needs to build a transparent and structured medical device reimbursement pathway, that will improve current practices and protocols concerning process, evaluation, data gathering and communication. Absent a significant increase in budget, authorities will continue to be faced with reimbursement trade-off decisions to improve patient access. However, improvement in patient care can also result in budgetary savings. A more structured dialogue among key stakeholders (regulatory agencies, government authorities, industry players, etc.) should be established to transparently work on improving health priorities, balancing expenditure and savings, and improving patient access — with the ultimate objective of ensuring access to innovative therapies while meeting fiscal constraints.
Structuring Unstructured Medical Device Reimbursement in India
Key Takeaways
Rising healthcare expenditure in a nation with a dominant low to middle income band population garners the need for a structured medical device reimbursement system to reduce out-of-pocket payments
The adoption of a comprehensive and transparent reimbursement pathway would require overcoming current challenges of unclear evaluation criteria and discord between the public and private sectors
Our proposed medical device reimbursement evaluation pathway entails a reassessment of current practices by establishing an open portal between the NHA and other stakeholders in healthcare for proposal submission of new therapies guided by clearly defined evaluation criteria for reimbursement consideration
Continuous dialogue among key stakeholders (regulatory agencies, government authorities, industry players, etc.) should be established to transparently work on improving health priorities, balancing expenditure and savings and improving patient access, with the ultimate objective of ensuring access to innovative therapies while meeting fiscal constraints.
Loading transcript...
Loading transcript...
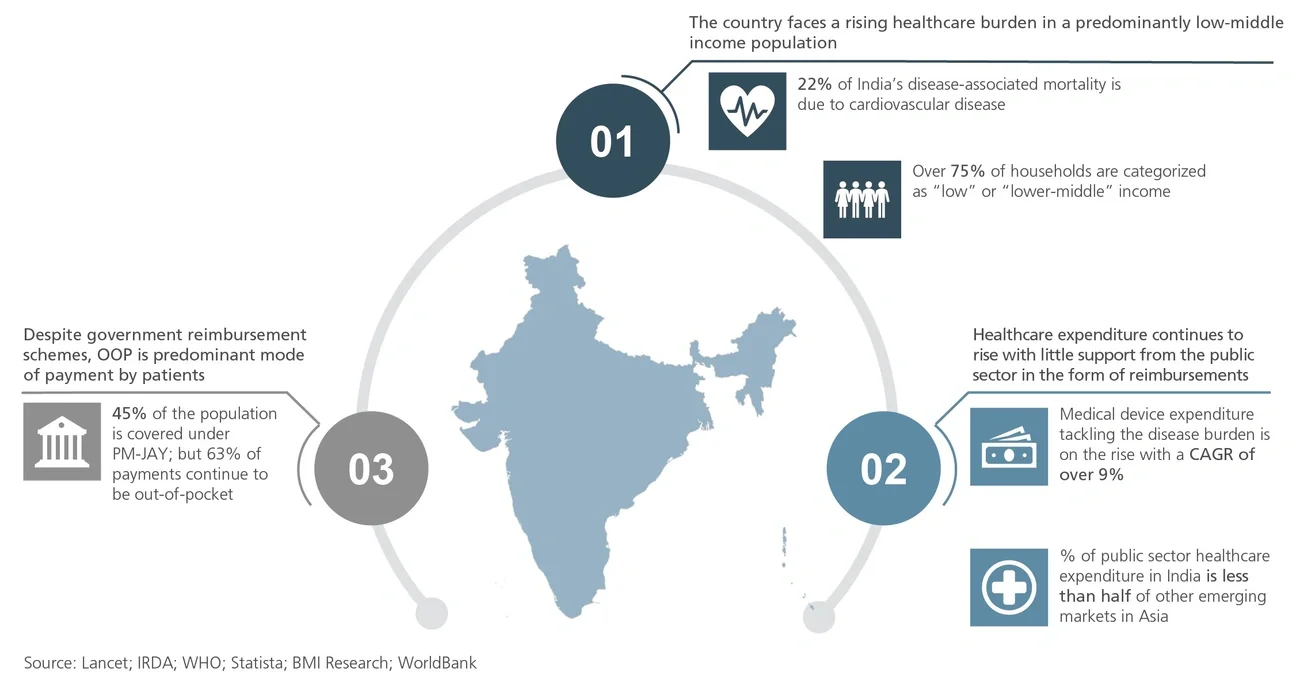
Healthcare expenditure on medical devices that address chronic conditions such as cardiovascular disease (CVD) has been rising sharply. Government healthcare spending in India currently accounts for only 27% of total healthcare expenditure; out-of-pocket payments (OOP) contribute the lion’s share (63%)1 In a predominantly low- and middle-income country, unaffordable OOP constrains healthcare access.
India’s payer landscape is fragmented, including over 30 private insurers and 17 separate government and employee schemes. Currently, 45% of the population is covered under government schemes.2 Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (PM-JAY), the largest of these, is a nationwide scheme providing health insurance for secondary and tertiary care hospitalization of Rs. 5 lakhs (~$7,000) per family annually. While the goal of providing the poorest 40% of the population with health insurance is laudable, nationwide implementation is a daunting challenge. Increasing the current disease coverage in PM-JAY can help improve the participation of hospitals.
Cardiovascular diseases constitute the highest disease burden in India; ischemic heart disease causes 22% of the nation’s disease mortality. Widely accepted and available tools and therapies like fractional flow reserve, implantable cardioverter defibrillator (ICD) and cardiac resynchronization therapy (CRT) have proven clinical and cost benefits. They deliver lower mortality, reduced risk of rehospitalization and shorter recovery times. And yet they are not included in the reimbursement lists of government insurance schemes. About 20% of cardiac implantable electronic device (CIED) implants in India are ICDs or CRTs. This compares to the 63% distribution of patients with heart failure or tachycardia (patients who require the devices).
Since OOP is not an option under PM-JAY, it is imperative that reimbursement lists are updated with therapies demonstrating clinical evidence of efficacy and societal benefit, including cost savings.
The adoption of a comprehensive, transparent and structured medical device reimbursement model in India will require the reassessment of several current practices and principles:
- Device cost is still the primary evaluation criteria in India, with too little emphasis on long-term patient outcomes.
- Publicly available information on the evaluation documents and the timelines for assessment are insufficient for essential stakeholder engagement.
- The absence of a documented, annual or fixed-interval review of reimbursement lists is a process limitation wholly insufficient to review all medical devices across 24 specialties for more than 1,000 health benefit packages.
- Limited resources with evolving technical skills are available to conduct structured Health Technology Assessments (HTAs), limiting the ability to obtain health economics data for newly introduced therapies.
- There are differences between private and public health stakeholders on the most appropriate evaluation framework of new therapies for inclusion in reimbursement lists, and discord further limits the implementation of government schemes in private hospitals.
- The under-representation of private hospital physicians in the nomination and review of novel therapies and medical device rates in reimbursement lists is sub-optimal.
Figure 1
Healthcare landscapes in India
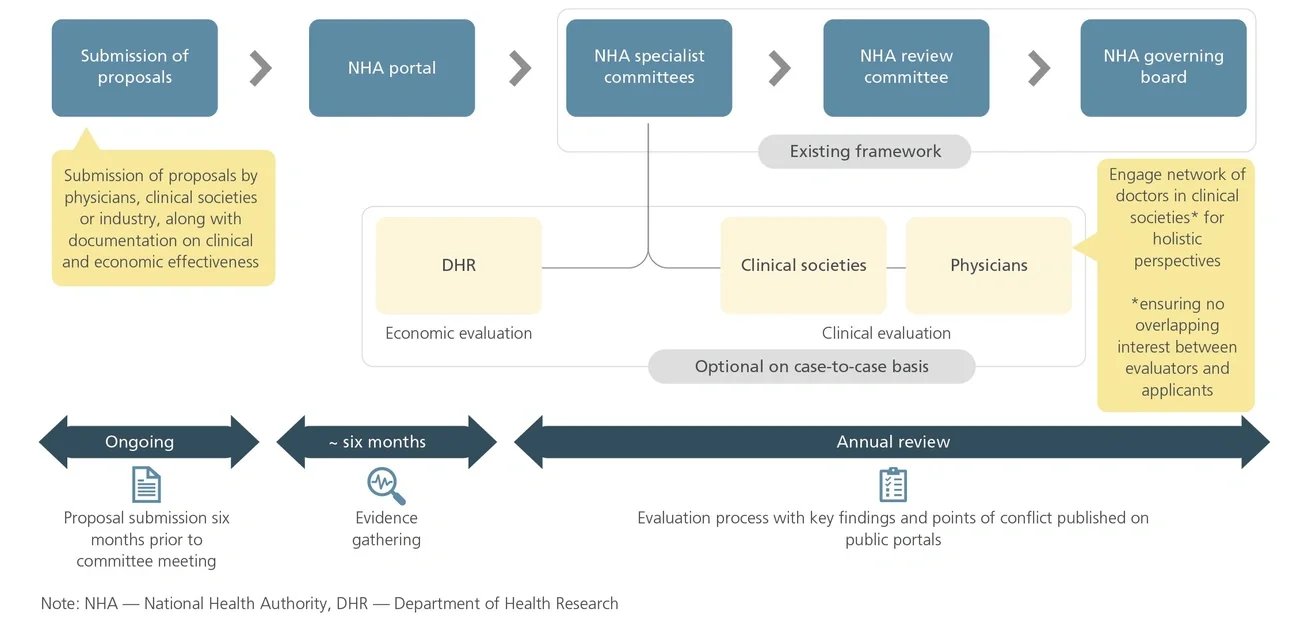
A National Health Authority (NHA)-owned portal would facilitate the submission of proposals by external stakeholders, including physicians, the medical device industry and clinical societies. A clear template for proposal submissions should include detailed documentation about the proposed therapy, including clinical efficacy and cost-effectiveness, product safety, the effectiveness of the solution in comparison to prevailing therapies, a current estimate of utilization (depending on disease incidence/prevalence) and the status of coverage by other insurance schemes, both public and private.
The NHA should engage clinical societies and the Department of Health Research (DHR), leveraging their expertise on clinical and economic data where additional evidence or documentation is required. A feedback loop should be established to convey the need for additional evidential submissions, if the documentation provided by physicians or other stakeholders is insufficient or incomplete.
Subsequently, proposals with sufficient validated clinical and economic evidence can be raised back to the specialists and review committees for further discussion and approval. With review committees convening annually to review reimbursement lists, a deadline for submitting the proposals should be set at least six months prior.
Key points of discussion in the review process, including any points of conflict, should be released on public domains, ensuring stakeholder alignment.
Figure 2
A proposed medical device reimbursement evaluation pathway
The limitations of the existing device reimbursement model can be addressed by lifting inclusivity in the process, emphasizing clinical and economic outcomes, facilitating greater deliberation and providing more transparency for all stakeholders.
- A more inclusive process: Create a pathway for submitting proposals to NHA expert panels, ensuring greater private hospital representation in these advisory panels for a genuinely holistic perspective.
- Rebalanced evaluation criteria: Rebalance the weightings assigned to (a) the clinical parameters — efficacy, recovery time, risk of rehospitalization, mortality, and QALYs gained, and (b) the anticipated economic outcomes — the cost-effectiveness of the healthcare intervention and impact on OPP.
- An open platform for data gathering and data sharing: Build a platform for the major stakeholders such as industry, clinical societies and physicians to share health economics data and clinical data on proposed therapies using portals for evidence submission to the NHA (the submitted documents can provide additional evidence if required to substantiate the nomination).
- Enhanced evaluation transparency: Enhance evaluation transparency by improving the availability of publicly shared information on the evaluation process, metrics and assessment timelines to better align all the relevant healthcare stakeholders.
Endnotes
1Final Global Health Database 2019.
2Insurance Regulatory and Development Authority.





