The confluence of several key trends in U.S. healthcare, including an aging population, shifts away from inpatient care, and a rise in healthcare consumerism has led to an increased emphasis on post-acute care, particularly care that permits aging in place.
By 2030, 1 in 5 Americans will be over the age of 65. This cohort makes up ~14% of the U.S. population but represents nearly half of the top decile of healthcare utilizers. Consumer demand for lower-cost healthcare and payer pressures (e.g., utilization management and value-based contracting (VBC)) are driving a migration from high-cost, inpatient care. Outpatient services as a share of overall hospital revenue increased from 28% in 1994 to nearly 50% in 2020. Given these macro trends, healthcare providers and investors are thinking more critically about post-acute care offerings, including palliative, hospice and home-based care.
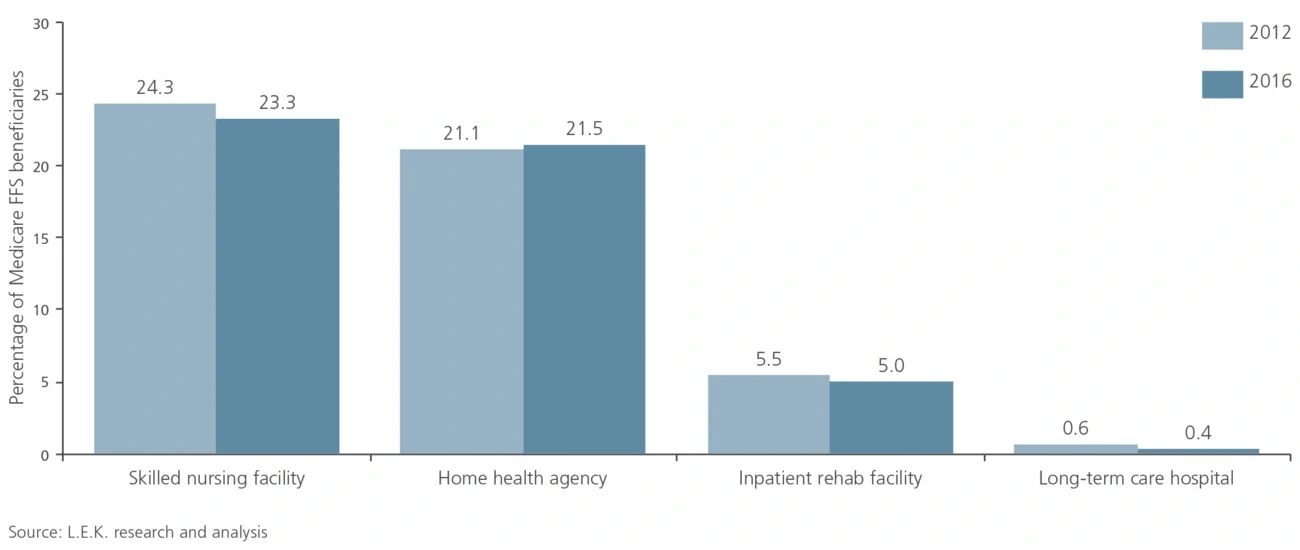
From 2012 to 2016, approximately 50% of all Medicare beneficiaries utilized some form of post-acute care within 90 days of a hospital discharge. While skilled nursing facilities represent the bulk of this 50% (see Figure 1), home health utilization is expanding, and it is positioned to become the top form of post-acute care within a few years. This follows an ongoing shift in patient and provider preferences toward home-based care: According to one 2017 survey conducted by the Kaiser Family Foundation, 7 in 10 Americans would prefer to die in their home. As a result, end-of-life care continues to gain acceptance and penetration.