NGS and big data are accelerating the biomarker innovation cycle
Against this backdrop, there is an acceleration in the biomarker innovation cycle driven by the comprehensive genomic profiling of tumors using NGS. L.E.K. Consulting estimates that 10-20% of metastatic patients receive NGS profiling in the U.S. today, and that number could increase two to three times in the next three to five years (which represents hundreds of thousands of patient cases annually).
Many of the NGS providers are building large data sets incorporating genomics and clinical and outcomes data, which is enabling identification and retrospective validation of new biomarker associations directly from real-world clinical cases. This activity has the potential to validate new biomarker associations backed by a significant number of patient cases (often dwarfing what is feasible with traditional clinical trials). Supported by this strength of evidence, it is expected that guidelines and clinical adoption of these biomarkers will follow quickly. Conceptually, this represents the application of big data in precision genomic medicine.
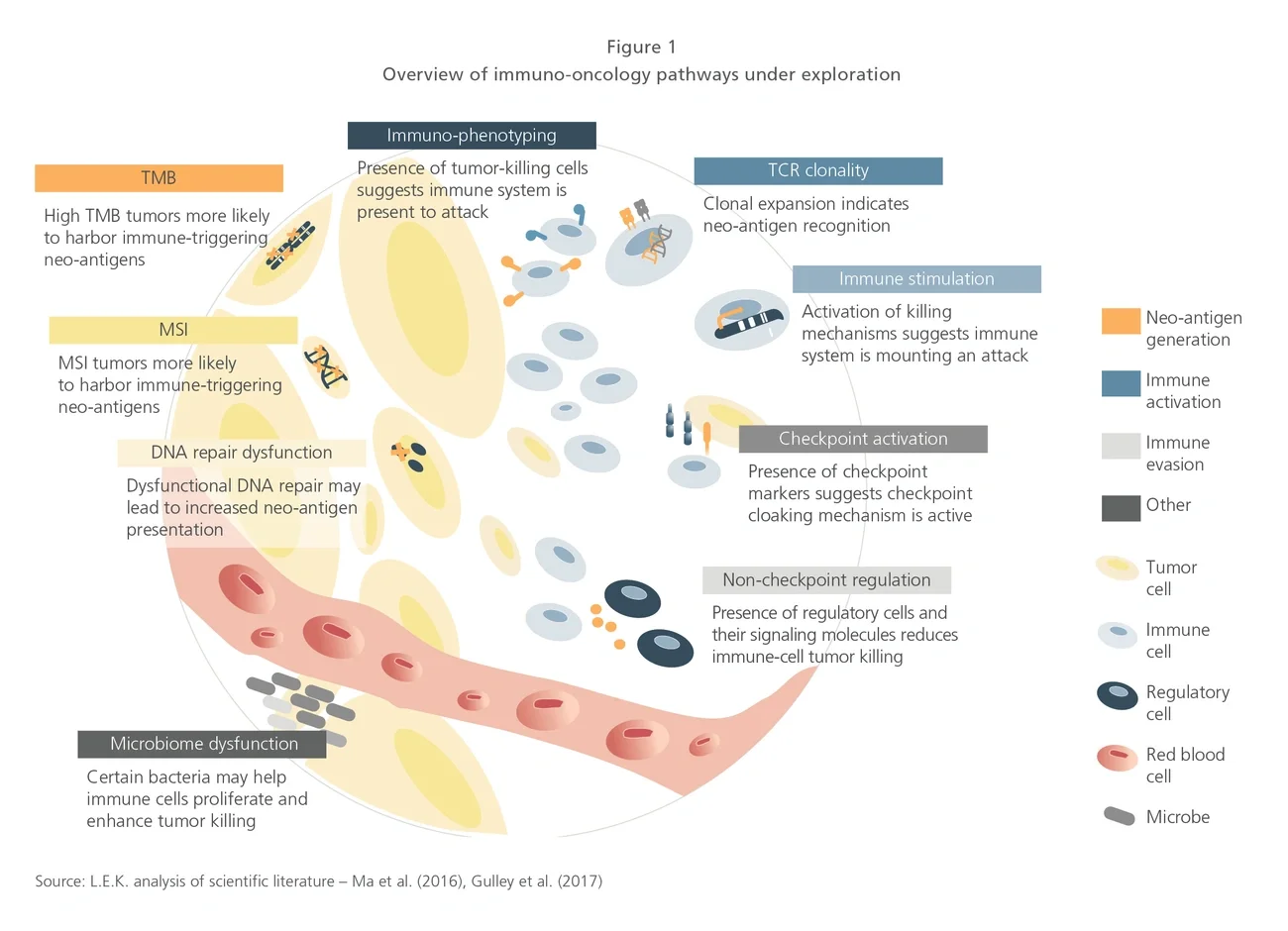
However, as highlighted earlier, this is no longer purely conceptual. The rapid rise of TMB represents a paradigm shift. TMB isn’t even a definable genomic biomarker in the traditional sense. TMB is not affiliated with a specific gene or pathway, but rather it is an observation that tumors with a relatively high frequency of mutations (high TMB) tend to respond better to checkpoint inhibitors (thought to be due to increased neo-antigen presentation). Interestingly, TMB also represents a new situation where diagnostics companies have forged the path and biopharma companies have followed suit. This stands in significant contrast to other targeted therapies where biomarkers and their associated complementary/companion diagnostics were largely validated by biopharma-sponsored pivotal trials.
TMB is also creating a virtuous discovery cycle that may only continue churning out new and more nuanced biomarker associations. NGS is required to measure TMB, and as TMB becomes more routinely adopted, it is an important driver to continued NGS adoption. Furthermore, NGS panel sizes continue to grow, and digitization of healthcare data by players such as Flatiron Health Inc. and COTA Inc. is enabling the creation of massive minable data sets.
The road ahead
There is a long road ahead for the immuno-oncology diagnostics space to mature. As discussed earlier, the science and supporting evidence need to be developed, and there are many directions in which they could go. Will it end with a reductionist biomarker strategy reliant on a few highly predictive biomarkers, or will it end with a more comprehensive biomarker strategy that looks at many pathways in concert? Certainly, the biology of immuno-oncology therapies, which relies on the interaction between a dynamic tumor and the immune system, suggests the more comprehensive strategy may prevail in the long run, but it will take time for that to materialize.
Separately, the industry needs to drive standardization, not only in pathways and biomarkers assessed, but also in defining standards around interpretation, including defining thresholds for what constitutes a biomarker-high or biomarker-positive result. Standardization and concordance across sample types assessed will also need to be worked out, including understanding cell heterogeneity (for both tumor and immune cells) and between tissue-based samples and those derived from biofluids, including CTCs, peripheral immune cells, cell-free components, exosomes and so forth.
The industry will also ultimately want to consolidate testing into a standard set and will not support a different test for every therapeutic option under consideration. This means there will need to be cooperation and collaboration across the industry, and looking at other diagnostics markets, a reasonable assumption suggests three to five major competitors will emerge as leaders. Access to novel diagnostic approaches will also need to be addressed. Today, many of the emerging immuno-oncology diagnostic tests require specialized instrumentation and operators, may take many weeks to process and are not well-reimbursed. Clearly, as the industry scales, this will need to change and fit better into therapeutic decision-making windows and healthcare economics.
Biopharmaceutical companies will need to adapt in this new high-paced biomarker environment. Trying to stay abreast of the biomarker landscape in a sequential fashion with each new biomarker approval may put companies into endless catch-up mode.
An alternative strategy could be to proactively assess multiple pathways and biomarkers at the outset, leveraging basket trials with fast conditional approvals to match therapeutic options to each patient’s unique (and ever-changing) biomarkers.
Organizationally, biopharmaceutical companies will need to change across many functions. Deeper embedding of biomarker/ diagnostics groups into development and commercial functions will be required. Business development activity with diagnostics partners will need to focus on broader collaborations with a focused set of diagnostic companies, with the ultimate goal of creating industry-standard diagnostic solutions. Market access and pricing functions will also need to consider how evolutionary biomarker strategies impact pricing and reimbursement of both the immuno-oncology diagnostics and therapeutics. Regulators will do well to enable such forward-thinking approaches. Just like the immune system, the industry needs to adapt to enable immuno-oncology companion therapies and diagnostics to reach their full potential.
Editor’s note: This article first appeared in In Vivo.