The biology is more connected than the market knows
A significant, and underappreciated, insight to emerge from recent women’s health research is that reproductive, cardiometabolic and immunological pathways in women are deeply entangled.
This entanglement is structural, not incidental. Estrogen actively regulates immune tone, vascular function and metabolic efficiency. Its decline at menopause does not simply produce reproductive symptoms — it triggers changes across cardiovascular, inflammatory and metabolic systems simultaneously. The hormonal transitions that define women’s reproductive lives — puberty, pregnancy, menopause — are systemic inflection points that alter disease risk and expression across multiple organ systems.
For large pharma companies with existing strengths in cardiometabolic systems or immunology, this is not complexity to manage — it is a strategic asset. The right assets, deployed against the right indications, can build compounding franchise advantages across what would otherwise appear to be disconnected disease areas.
The GLP-1 opportunity: Female-specific obesity phenotypes
Approximately 38 million postmenopausal U.S. women are overweight or obese — it’s a patient population that is large, treatment-seeking and biologically distinct from the populations on which landmark anti-obesity trials were built.
Menopause creates a specific metabolic phenotype. Estrogen decline drives central adiposity, reduces energy expenditure and impairs fat oxidation in ways that fundamentally alter a woman’s responsiveness to standard anti-obesity therapy. Yet the SURMOUNT and SCALE trials — the landmark studies defining GLP-1 efficacy — were not powered to detect menopausal effects. The menopausal phenotype that drives a significant share of female obesity burden was effectively invisible to the science that defined the standard of care.
Emerging evidence suggests this gap is commercially meaningful. A 2026 Mayo Clinic retrospective cohort study (Castaneda et al.) found that among 120 postmenopausal women treated with tirzepatide, those receiving concurrent menopausal hormone therapy (MHT) achieved approximately 19.2% total body weight loss compared to the 14% of matched nonusers. MHT may function not merely as symptom relief but as a metabolic amplifier — restoring the hormonal context in which GLP-1 therapy operates. (Observational, n=120; randomized controlled trial (RCT) needed.)
For companies with GLP-1 assets, the commercial logic is direct. Postmenopausal obesity is a large, biologically differentiated indication with a clear OB-GYN call point. Women already account for an estimated 65%-75% of current anti-obesity medication use.² A company that designs sex-stratified trials, builds prescriber relationships with ob-gyns and develops evidence for combination approaches in this population will generate data that general-purpose GLP-1 development cannot replicate — and that positions its assets as purpose-built for the majority of patients already using them.
PMOS: 15 million patients, no approved mechanistic therapy
Between 5 million and 10 million U.S. women have PMOS,³ making it one of the most prevalent endocrine disorders in the country and one of the most underserved. PMOS is not a single-pathway disease. At its core, PMOS is a self-reinforcing cycle between insulin resistance and androgen excess, amplified by chronic low-grade inflammation. The current standard of care (oral contraceptives, metformin, lifestyle modification) addresses symptoms without disrupting this cycle. No approved therapy directly targets either of its two primary drivers.
The first company to treat the disease rather than simply manage its symptoms will not displace an established competitor. It will define the standard of care.
GLP-1-based therapy is the nearest-term credible path into that space. In an RCT, liraglutide improved hyperandrogenism and menstrual cycle frequency versus a placebo in women with PMOS.⁴ Across studies, GLP-1 receptor agonists have shown reductions in free testosterone and improvements in sex hormone-binding globulin, endocrine effects that extend beyond metabolic control. These findings largely emerged as secondary outcomes from trials not designed to test them. No large RCT has yet been powered to detect PMOS-specific endocrine endpoints with semaglutide or tirzepatide. That is the evidentiary gap and the commercial opportunity.
Androgen excess is the second, largely unaddressed, vector. Hyperandrogenism is a defining feature in the majority of PMOS patients, yet no approved therapy directly targets androgen production (combined oral contraceptives indirectly lower androgen levels). Current approaches suppress symptoms without reaching the source. Early-stage research is beginning to identify the biosynthetic pathways involved, but this remains a genuine area of mechanistic white space.
PMOS and postmenopausal obesity share a natural call point in OB-GYN. Investment in prescriber relationships, market education and diagnostic infrastructure built around one compounds directly across the other.
Autoimmune disease in women: A market built without female biology
The autoimmune market is, in many ways, a women’s health market, given the high prevalence in women of many major autoimmune diseases. Eighteen of the top 20 autoimmune diseases are overrepresented in female patients, yet the field has been developed largely without accounting for why.⁵
Two biological mechanisms are central. Immune cells express estrogen, progesterone and androgen receptors; hormonal shifts alter immune activation thresholds and influence disease onset and activity across a woman’s life. Separately, incomplete X-inactivation in immune cells leads to the overexpression of innate immune-regulatory genes, including TLR7 and TLR8, creating a structural predisposition toward hyperactivated immune responses.⁶ Emerging evidence links the degree of incomplete X-inactivation with disease severity in systemic lupus erythematosus (SLE) and Sjögren’s disease. While still in the early phases of research, this biology points to a novel disease-modifying frontier that current autoimmune therapies do not directly address.
The first commercial opportunity is in diseases where women are the predominant patient population and where sex-specific biology measurably shapes disease course. In SLE and Sjögren’s, hormonal status influences flare frequency and long-term disease trajectory. In rheumatoid arthritis, sex differences in onset, severity and treatment response are well documented but have not driven drug development. The opportunity is not simply to incorporate these variables into trial design. It is to develop therapies that directly target these mechanisms: drugs that modulate hormonal-immune cross talk or address the X-chromosome-driven immune hyperactivation implicated in disease severity. These represent new mechanisms in indications that have been studied for decades through a sex-agnostic lens.
The second opportunity is in conditions specific to women where the underlying mechanism is immune and inflammatory. Endometriosis — driven in part by peritoneal immune dysfunction, with IL-1 β, IL-6 and TNF-α implicated in microenvironment inflammation — is a clear example. Historically managed hormonally or surgically, this condition has not been the subject of inflammation and immunology (I&I) drug development. The therapeutic approaches proven across I&I, targeting cytokines, inflammatory pathways and immune cell function, have not been applied here.
Both opportunities share a common foundation — drug development built around sex-specific biology — and together define a position in women’s immunology that existing autoimmune programs are not structured to occupy.
What it takes to win
The strategic case for women’s health is clear, but the execution requirements are demanding. Winning in women’s health will require a distinctive set of capabilities that go beyond standard pharma launch execution.
Market building at scale
Two of the most attractive near-term women’s health indications, postmenopausal obesity and PMOS, share a structural characteristic: The patient populations are substantially larger than current diagnosis rates suggest. PMOS in particular is chronically underdiagnosed. First-mover advantage in these indications will depend not only on having the right asset but also on investing ahead of the market to create the diagnostic and prescriber infrastructure that makes the market real.
OB-GYN as a strategic call point
The OB-GYN call point has historically been treated as a niche by large pharma companies oriented around primary care or specialty medicine. That calculus is changing. The ob-gyn is uniquely positioned at the intersection of reproductive health, metabolic disease and preventive care and, for many women, is their primary or sole physician contact. Building deep, durable relationships with this prescriber base is not just a launch tactic; it is the foundational infrastructure for a women’s health franchise.
Sex-specific trial design
Companies that design trials with menopausal status, hormonal biomarkers and reproductive life stage as first-order variables rather than demographic afterthoughts will generate evidence that competitors cannot easily replicate and that positions their assets as purpose-built for female patients.
The window is open — for now
The women’s health market is not a future opportunity. It exists today, in the form of tens of millions of patients with inadequately treated conditions, a competitive landscape with no integrated leader, and a scientific base that is maturing rapidly. The question is which company will move first and with enough conviction to build the market, not just enter it.
For companies with established strengths in cardiometabolic medicine and immunology, the path is more accessible than it may appear. The biology points to the same call point. The commercial infrastructure compounds across indications. And the window for first-mover advantage, while open for now, will not stay open indefinitely.
For more information, please contact us.
Note: AI was used in the drafting of this piece.
L.E.K. Consulting is a registered trademark of L.E.K. Consulting LLC. All other products and brands mentioned in this document are properties of their respective owners. © 2026 L.E.K. Consulting LLC
Endnotes
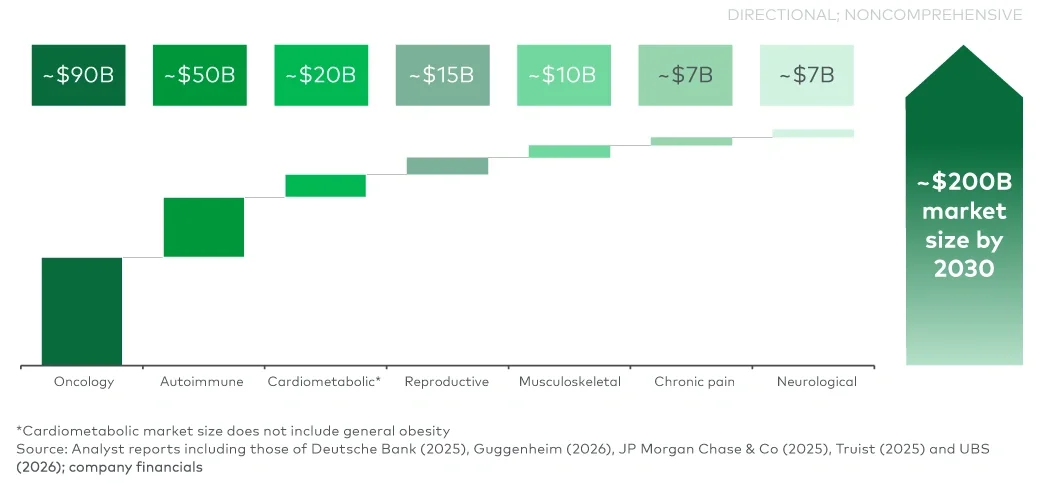
¹L.E.K. analysis of Guggenheim, Barnes, Deutsche Bank and UBS analyst reports and Delve Insights, The Business Research Company and Grand View market reports.
²Cite Real Chemistry (IRIS, 2025), bioRxiv preprint (Donofry et al., 2025). 6WHO (2026); Endocrine society; Yu et al. Am J Obstet Gynecol (2023).
³WHO (2026); Endocrine society; Yu et al. Am J Obstet Gynecol (2023).
⁴Nylander et al. Reprod Biomed Online (2017); Elkind-Hirsch et al. Fertil Steril (2022).
⁵Abend et al. J Clin Invest (2025).
⁶Souyris et al. Sci Immunol (2018).