



Key takeaways
-
The U.S. healthcare industry is facing a range of issues, including soaring medical costs, clinical variation and health outcomes that underindex those of other developed nations.
-
Medical care alone accounts for just 10%-20% of health outcomes; 80%-90% is dictated by environmental and social factors, or “social determinants of health” (SDOH).
-
Holistic approaches to care that incorporate SDOH are needed to effectively address both current and future health challenges.
-
L.E.K. Consulting has developed a framework that can help industry stakeholders build an effective SDOH strategy.
Skyrocketing medical costs, clinical variation and outcomes that underindex those of other developed nations have risen to the forefront as key issues facing the U.S. healthcare industry. Consequently, payers, at-risk providers, health-focused nonprofits, government entities and many other healthcare organizations are investing in strategies and solutions aimed at delivering high-quality care at lower cost and are increasingly focused on preventive care measures that improve population health.
However, medical care alone accounts for just 10%-20% of health outcomes; the remaining 80%-90% is dictated by environmental and social factors, or “social determinants of health” (SDOH).1 As such, healthcare organizations are increasingly prioritizing SDOH-focused solutions — either as part of a larger population health strategy to lower total cost of care (e.g., for at-risk entities like payers and accountable care organizations) or in service of organizational missions to reduce health inequity among member and patient populations.
The initial COVID-19 period has only increased the urgency for SDOH-based population health solutions. Anecdotal evidence and preliminary data indicate that social and environmental factors (housing insecurity, for instance) predispose individuals to infection. Further, the success of key mitigation tactics — testing, contact tracing and isolating infected/exposed individuals — has proven highly dependent on meeting an individual’s social health needs. Isolation requires stable housing in which to quarantine, access to food and the economic resources to weather potential income loss. Holistic strategies that incorporate SDOH are needed to effectively address both current and future health challenges.
Despite making SDOH a priority, many healthcare organizations struggle with where to begin. Social determinants are numerous and interdependent, and the sheer volume of systemic deficiencies driving adverse health outcomes can be overwhelming. Based on years of experience assisting healthcare organizations of all types in prioritizing and focusing their efforts for maximum impact — from payers and providers to healthcare IT companies to healthcare-focused nonprofits — L.E.K. Consulting has developed the following framework for an effective SDOH strategy.
Who, where and what?
Often, the best way to start is with a small pilot that can be refined and scaled over time. Pilots are designed by answering three questions: whom to serve, where to locate and which needs to address first. The most effective SDOH strategies address the unique and specific needs of a defined population and are geographically focused.
Focus will increase an organization’s time to impact. The needs of the target population can be varied. Healthcare organizations, particularly those involved in the direct provision of care with finite resources, should initially choose no more than a handful of social needs to focus on while perfecting their SDOH strategies.
Focus will also enable organizations to integrate and optimally deploy the vast amounts of funding and numerous community resources that already exist at the local level. Federal funding for social supports (not including state and local funds) totals roughly $1.4 trillion nationally, far exceeding what any single healthcare organization might contribute. And local social- and health-focused organizations often number in the thousands. Fragmented funding streams and lack of coordination limit their ability to make meaningful change; the best SDOH solutions organize and enhance what already exists at the local level.
Step 1: Define a focus population
Organizations should choose a population whose characteristics align with their overarching objectives. For example, if an organization’s goal is to lower total cost of care, it could choose to focus on the top 5%-10% of the most costly patients or members on an annual basis. Alternatively, if the primary goal is to reduce healthcare disparities in a particular geographic area, then the organization could identify patients with the worst health outcomes from among the local population, controlling for factors such as demographics and disease state. How broadly or narrowly an organization chooses to define the focus population will ultimately depend on the resources it has available to execute a pilot, as well as its unique strategic priorities and positioning.
Step 2: Establish the geographical scope
An individual’s SDOH are highly dependent on their local environment, social network and access to local resources. To be successful, an SDOH strategy must be tailored to the needs of the focus population within a contained geographic region. To that end, successful SDOH strategies often leverage established local organizations and processes to engage the focus population. Consider a situation where a Managed Medicaid payer seeks to increase the number of children enrolled in its plan who receive a well-child visit. Transportation barriers, the challenges of taking time off work, a lack of stable housing and numerous other factors prevent parents from bringing their children to a pediatrician. To circumvent those barriers to accessing preventive care, the payer could arrange to bring a pediatrician to the local public school — which already has strong community connections and is embedded in children’s daily routines — once a week. Such a strategy is inherently geographically focused and would require forging a close partnership with the school.
Further, as it does with its focus population, a healthcare organization must align the geographic scope of its SDOH strategy with its overarching objectives. For example, if its objective is to improve health outcomes, the organization could target local service areas with high member/patient density and particularly poor outcomes. Of course, this requires robust data, and often organizations lack internal data to fully characterize the demographics and health status of their focus population (e.g., health systems that are limited to the data contained within their electronic medical records (EMRs)). In such cases, a geography-driven prioritization exercise utilizing publicly available data sources can be effective. L.E.K. employs a geographic prioritization methodology grounded in the peer-reviewed County Health Rankings methodology and adjusted for data availability at the most granular level (ZIP code) (see Figure 1).
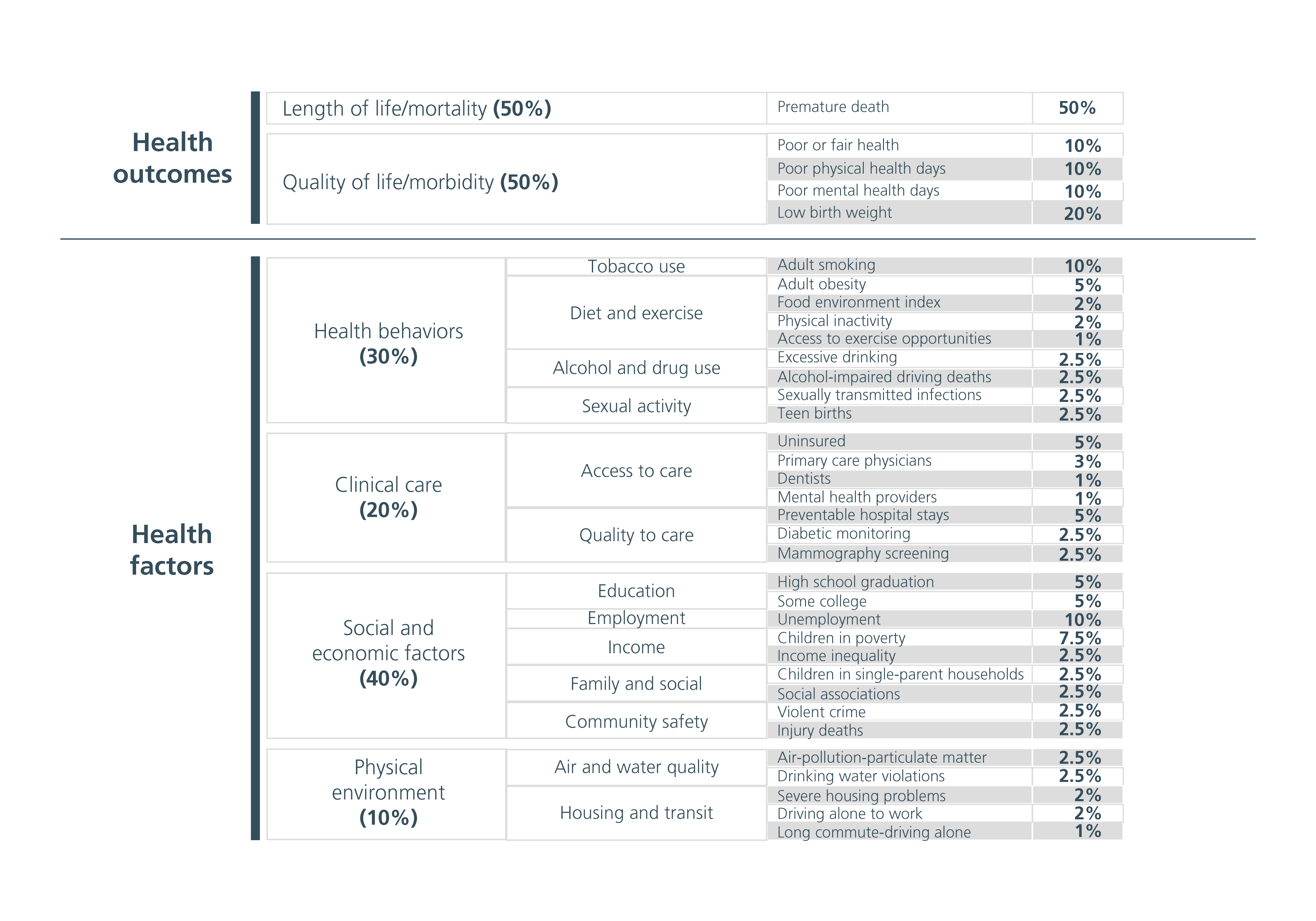
It is important to keep in mind that a target geography will not always align perfectly with externally defined geographic units (e.g., ZIP codes or counties). An actionable geographic definition will take into account geospatial elements that impact movement and access (highways, bridges, etc.) and align with local neighborhood definitions. Therefore, healthcare organizations should collect data at the lowest possible level of granularity — preferably at the ZIP code or even census tract level — to facilitate a preliminary prioritization and then adjust their definitions for real-world applicability.
Step 3: Identify and prioritize root-cause SDOH for action
Once an organization defines its focus population and geography, it must describe the underlying demographic, socioeconomic and health characteristics, as well as the root-cause drivers of adverse health outcomes, in as much detail as possible. Doing so will enable targeted and actionable strategies. Secondary data, such as payer enrollment files, claims data, EMR data and publicly available sources, provides a baseline from which to develop informed hypotheses. But to truly understand and internalize the root-cause social and environmental drivers of adverse health outcomes, organizations must engage in conversations with local market participants that interact with the focus population, such as social workers, food banks and homeless shelters.
For example, secondary data may show that the focus geography is a food desert, lacking easy access to a grocery store stocking fresh produce. By having conversations with local market participants, organizations may discover that the reason the area is a food desert is that the local population’s Supplemental Nutrition Assistance Program (SNAP) benefits are insufficient to cover the cost of healthy and nutritious food. They may further learn that members of that population have strong personal ties to the local convenience store where they shop for food. Solving transportation challenges is therefore not enough. Understanding root-cause drivers of health outcomes will help organizations develop effective and actionable strategies.
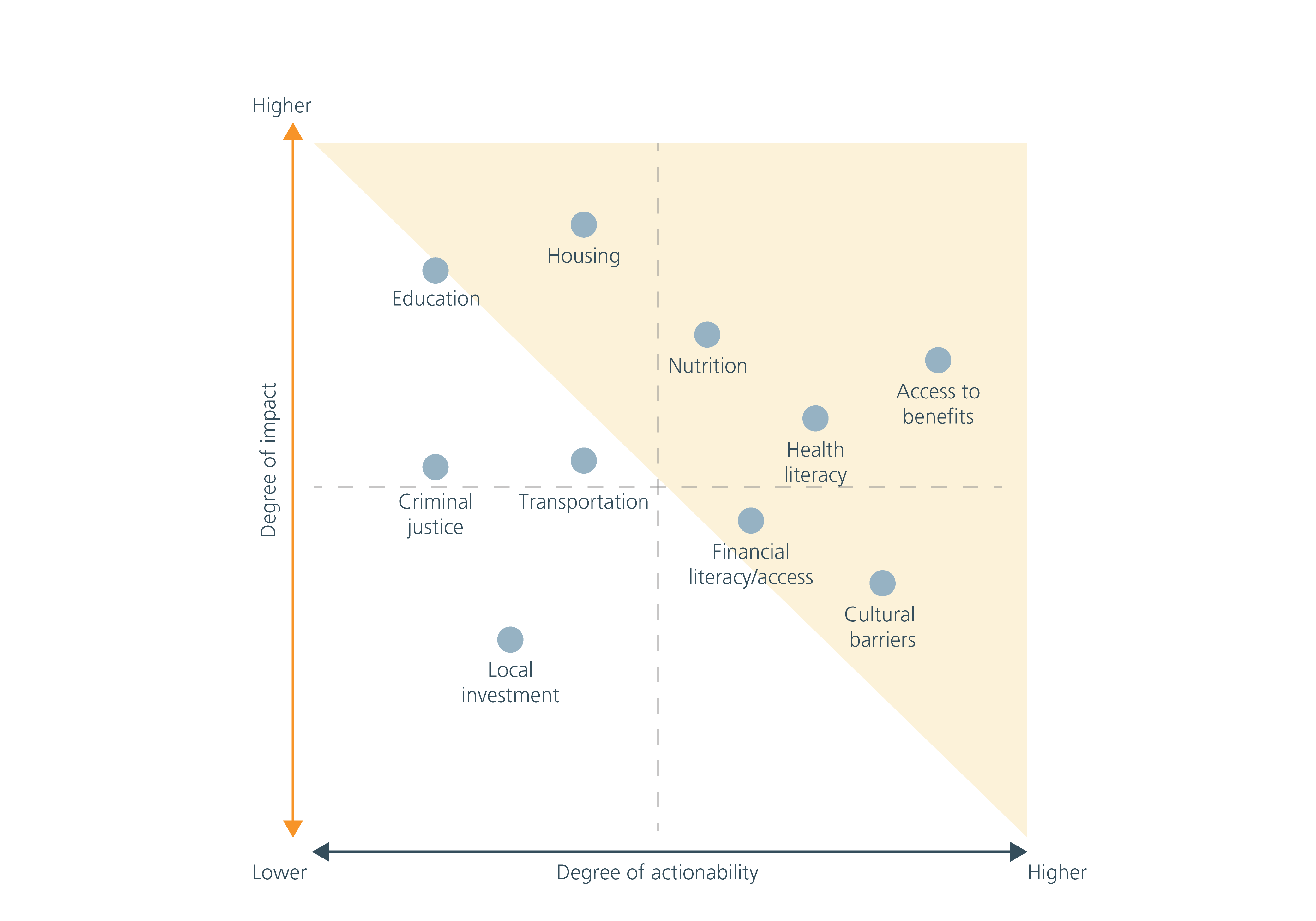
Once the root causes of adverse health outcomes are identified, healthcare organizations will likely find these causes are numerous. And with limited resources, it is nearly impossible to address all of them at once. Thus, the next step is to prioritize root causes with the greatest impact on the factors they want to influence (health outcomes, cost, access, etc.) and are most closely aligned with the organization’s core competencies. For example, while a lack of education or high rates of crime will impact an individual’s physical and mental health, they may not be actionable by a healthcare organization. Rather, government policy and the efforts of other local and national organizations are likely the best way to address them. Similarly, embedded structural and policy barriers to expanding affordable housing stock in the local market, such as limited Department of Housing and Urban Development vouchers and long waiting lists, may stymie the ability to provide affordable housing to patients/members (although, if an organization has the capital and capabilities to invest in its own housing stock, this can be a very effective way to impact a key SDOH; Kaiser, for example, is investing up to $200M to address housing instability and homelessness) (see Figure 2).
Guardrails for successful SDOH solution implementation
These parameters — who, where and what — will help healthcare organizations focus and align their efforts with their strategic priorities. Beyond this framework, there are a few guardrails that are useful when implementing community-based solutions.
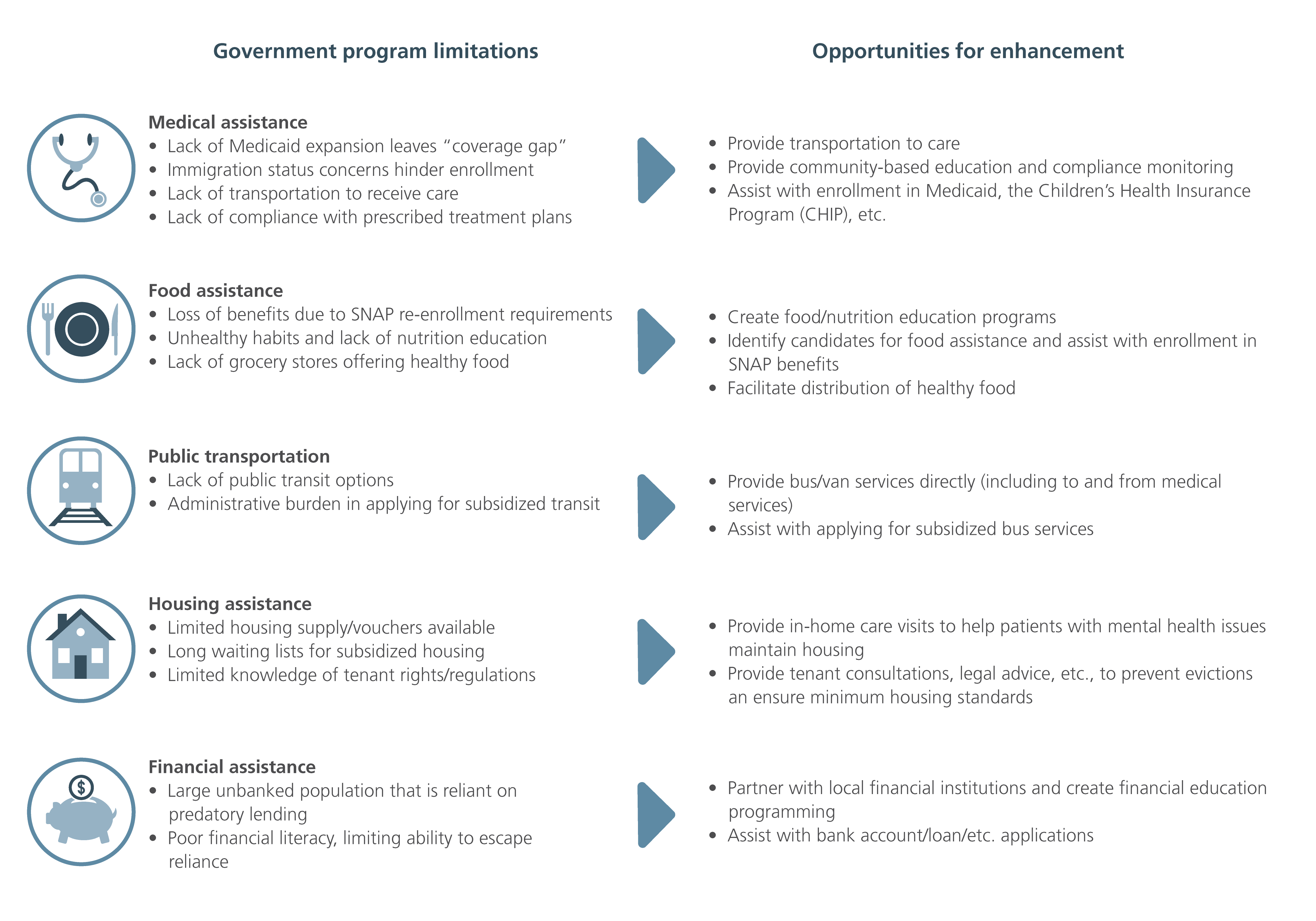
Be the glue that binds. There are myriad resources in existence today aimed at addressing SDOH; the federal government already spends some $1.4 trillion on social welfare programs, even before accounting for state and local government funding for Medicaid, public education and local infrastructure. However, the delivery of these programs is fragmented, and it can be difficult for beneficiaries to enroll in and stay enrolled in assistance for which they are eligible.
Take SNAP (food stamps), for example. Enrollment in the SNAP benefit can be challenging for several reasons: SNAP offices may be open only for a limited number of hours a day, requiring time off from work to apply in person. Applicants may lack access to a car or other mode of transportation. Documentation requirements can be confusing. Once enrolled, a beneficiary may lack access to a grocery store that stocks healthy and affordable food items. All these structural barriers limit the program’s ability to fully alleviate the impact of poor nutrition on health outcomes. To maximize the impact of their investments, organizations should develop solutions that do not try to duplicate what already exists, but instead fill these structural gaps and improve the effectiveness of government programs already in place.
In addition to government-funded programs, there are typically numerous existing local nonprofits and socially oriented providers in any given neighborhood that aim to address SDOH. However, they lack the resources, funding and/or coordination to expand their impact. Rather than creating an entirely new solution from scratch, it is often more beneficial for healthcare organizations to identify winners from among local organizations and help them improve and scale up.
Conversations with local service organizations are often invaluable in understanding where these programs and local organizations fall short, and in developing effective solutions that “glue” resources together (see Figure 3).
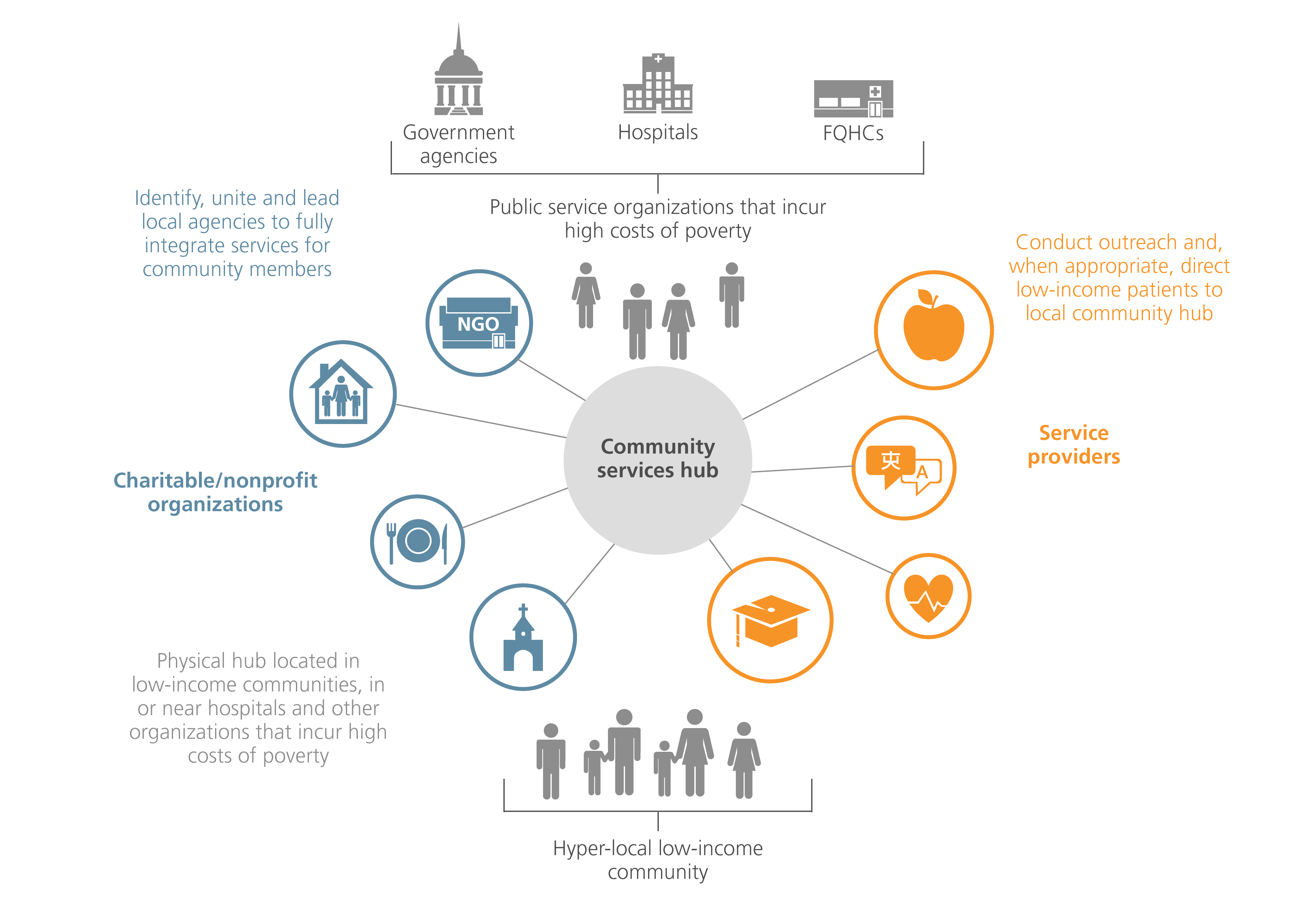
Pick an effective anchor partner. Strong relationships and frequent touch points with the focus population are key to an effective SDOH strategy. Organizations can seek to partner with a local “anchor” whose physical and/or virtual locations are embedded in the focus population’s daily habits and has already established credibility and strong connections with the local community. Possible partners include local schools, community centers and clinics (e.g., Federally Qualified Health Centers (FQHCs)). Using this anchor as a hub, organizations can link in services and solutions that lead to improved health outcomes (see Figure 4).
Carefully measure return on investment (ROI). To ensure the ultimate success of an SDOH pilot, organizations need to establish realistic but aggressive outcomes targets, track progress against these goals, identify barriers to achieving them and refine the operating model for continuous improvement. Doing so will yield a robust and scalable model, as well as valuable learnings to leverage for expansion into new populations and geographies. Further, doing so will demonstrate the proof of concept required to rally the organizational support and resources that will allow them to strategically expand.
SDOH are certain to play a growing role in future care models and operations for healthcare organizations. Those organizations that prove successful will orient their SDOH strategies to overarching goals. Using these goals as a guidepost, organizations must develop focused and hyperlocal pilots, with a defined population, geographic scope and set of social issues to be addressed. They must leverage the resources and funding already in place, seeking to connect and organize rather than duplicate existing efforts. Further, they must identify effective partners and diligently track and measure ROI to adjust the strategy for new learnings on an ongoing basis. Doing so will enable these healthcare organizations to achieve their overarching objectives and begin to address the more intractable problems that impact population health.
Endnote
1Hood, C. M., K. P. Gennuso, G. R. Swain, and B. B. Catlin, “County Health Rankings: Relationships Between Determinant Factors and Health Outcomes,” American Journal of Preventive Medicine, 50(2):129-135, 2016

09222020120925